Your regular diet may include traditional white rice. But what if we told you that you could choose a healthier type of rice? Yes, you heard correctly! Asia has traditionally grown rice, which is cultivated in a variety of colours and one of them is known as black rice. They are nowadays gaining popularity because of their beneficial properties, and nutritional value.
If you’ve ever had black rice, you can appreciate its unique purple-black colour, chewy texture, nuttiness, and slightly sweet flavour. But this special rice is more than just delicious; it’s also remarkably healthful, and it’s been recognized as a rice ‘superfood’ in recent years.
Black rice has a higher concentration of minerals like vitamin E, calcium, and potassium that support healthy bodily functions. Compared to other types of rice, it has higher levels of protein, fibre, and iron as well as high levels of amino acids and antioxidants which are beneficial for overall well-being.
Improves eye health
Black rice contains the antioxidants anthocyanin and vitamin E that promote eye health. Lutein and zeaxanthin, the two most significant carotenoids, are found in black rice that has been said to support and boost eye wellness. A nutritious diet rich in antioxidants and carotenoids also helps protect eye cells from the harmful effects of UV radiation. They are also important in terms of preventing eyesight problems with sight loss due to ageing.
Helps in weight loss
Black rice is a good source of protein and fibre, which can aid in weight loss by decreasing appetite and enhancing the feeling of fullness. According to research, people who consumed a combination of brown and black rice up to three times per day on a calorie-restricted diet were seen to lose significantly more body weight and body fat than those who only consumed white rice.
The presence of phenolic compounds present in black rice helps lower the rate of type 2 diabetes. The phenolic chemicals in black rice may be affected by the pancreatic and intestinal enzymes that break down sugars. This may result in lower blood glucose levels and a decreased risk of type 2 diabetes.
Has anti-cancerous properties
Anthocyanins from black rice help to reduce the number of human breast cancer cells and their growth and ability to spread. According to research a higher intake of anthocyanin-rich foods is connected with a lower risk of colorectal cancer and is also beneficial for overall well-being.
Good for the heart
Your ability to control heart conditions like hypertension and atherosclerosis may be improved by including black rice in your daily diet. Black rice consumption on a regular basis may help you lower cholesterol levels and blood vessel inflammation. Additionally, it also helps to lower blood pressure levels.
Good for hair and skin
The strong antioxidant level of black rice makes it great for your hair. Aside from that, it includes vitamins and minerals that are necessary for promoting hair growth and adding lustre to your hair.
According to experts, the high antioxidant content in black rice protects skin cells against oxidative damage. It helps treat skin conditions like acne, pimples, and other inflammatory skin conditions as well as skin ageing.
Final thoughts
Back rice is most likely the healthiest type of rice in the market. It has enormous nutritional value, which has a variety of positive effects on your health. Almost every organ in your body benefits from regular consumption of black rice. It improves mental skills and is good for the liver, eyes, heart, and respiratory system. It has some anti-ageing properties as well.
Furthermore, it promotes weight loss and helps in managing diabetes effectively. It is simple to add black rice to your everyday diet because of its simple cooking process. It is therefore advisable to include this grain in your diet due to its high nutrient profile, and numerous health advantages.
It’s all fun and games until you’re naked in a bathroom stall.
Sharee Miller is the author of Princess Hair and Don’t Touch My Hair. She lives in Jersey City with her spouse, toddler son, and two cats, Pumpkin and Spice. Her comics celebrate Black joy and self-care.
(PORTLAND, Ore.) — Oregon is set to become the first state in the nation to cover climate change expenses for certain low-income patients under its Medicaid program as the normally temperate Pacific Northwest region sees longer heat waves and more intense wildfires.
The new initiative, slated to take effect in 2024, will cover payment for devices such as air conditioners and air filters for Medicaid members with health conditions who live in an area where an emergency due to extreme weather has been declared by the federal government or the governor’s office, according to the Oregon Health Authority.
It aims to help people “dealing with the impact of extreme heat, wildfires and other catastrophes caused by climate change,” OHA director Patrick Allen said.
The measure is part of what the Centers for Medicare and Medicaid Services, of the U.S. Department of Health and Human Services, described as “groundbreaking Medicaid initiatives” in Oregon and Massachusetts.
The federal agency on Wednesday renewed Medicaid waivers for both states. Those waivers will cover non-medical services such as food and housing assistance for people with clinical needs in a bid to tackle the underlying social issues that can cause poor health.
Oregon will receive $1.1 billion in new federal funding for the new Medicaid initiatives covering climate change, nutrition and housing, described as “health-related social needs” by health officials. The state will pilot the changes over the next five years.
“Health care does not occur in a vacuum—it’s clear that we must look beyond a traditional, siloed approach to truly meet the needs of people, particularly those experiencing complex challenges,” Oregon Gov. Kate Brown said in a statement.
Massachusetts Gov. Charlie Baker said his state will “continue to implement innovative reforms that provide quality care, better health outcomes and equity.”
Oregon’s new Medicaid plan stands out for two first-in-the-nation policies: its climate change coverage, and a measure that will keep children continuously enrolled in Medicaid until age 6 without families having to re-enroll every year.
Officials in the Pacific Northwest have been trying to adjust to the likely reality of more intense heat spells following the region’s fatal “heat dome” weather phenomenon that prompted record temperatures and deaths in the summer of 2021.
About 800 people died in Oregon, Washington, and British Columbia during the heat wave as temperatures soared to an all-time high of 116 Fahrenheit (46.7 Celsius) in Portland and smashed heat records in cities and towns across the region. Many of those who died were older and lived alone.
In addition to covering payment for devices that maintain healthy temperatures and clean air inside the home, Oregon’s new Medicaid plan will also cover generators in the case of power outages.
“It’s based on the medical indication that you’re particularly vulnerable to heat events, or you have medical devices that are tied to being powered, or sensitive to smoke,” Allen said.
Oregon Medicaid members with health conditions will become eligible for such devices if they live in an area where an emergency due to extreme weather has been declared.
Climate change can pose risks to health, including heat-related illness during heat waves. Extreme weather events such as storms and floods can also negatively impact health, both physical and mental, and disrupt food systems. The risks disproportionately affect low-income communities, older people and those with underlying health conditions.
Medicaid is the federal-state health care insurance program that helps pay for health care for low-income people of any age. Each state determines eligibility and the full scope of services covered. The federal government reimburses a percentage of the state’s expenditures.
“There’s lots of discussion in climate change about making sure that as we address the health risks of a changing climate, that we do so in a way that reduces inequities,” said Kristie Ebi, professor in the Center for Health and the Global Environment at the University of Washington.
Oregon’s Medicaid initiative “is an opportunity to reduce some of those inequities for people who can’t afford, for example, a generator to make sure that life-saving equipment continues to run during heat waves,” Ebi said.
As for Medicaid coverage of food and housing assistance, Oregon and Massachusetts are expanding eligibility for such services.
Food support can include tailored meal plans based on health needs and Medicaid-funded prescriptions for fruits and vegetables. Housing services can include rental application assistance, moving help and eviction prevention.
Massachusetts will provide additional meal support for Medicaid members who are children or pregnant women with special clinical needs, according to the Centers for Medicare and Medicaid Services.
In Oregon, people experiencing life transitions, including those experiencing or at risk of homelessness, can be eligible for rental assistance for up to six months.
____
Claire Rush is a corps member for the Associated Press/Report for America Statehouse News Initiative. Report for America is a nonprofit national service program that places journalists in local newsrooms to report on undercovered issues. Follow her on Twitter @ClaireARush.
David Cave, a recovery coach who is part of an addiction specialty team at Salem Hospital, north of Boston, stands outside the emergency department.
Jesse Costa/WBUR
hide caption
toggle caption
Jesse Costa/WBUR
David Cave, a recovery coach who is part of an addiction specialty team at Salem Hospital, north of Boston, stands outside the emergency department.
Jesse Costa/WBUR
Marie lives in the coastal town of Swampscott, in Massachusetts. Last December, she began having more and more trouble breathing. One morning, three days after Christmas, she woke up gasping for air. A voice in her head said, “You’re going to die.” Marie dialed 911.
“I was so scared,” Marie said later. Describing that day, the 63-year-old’s voice filled with tension, and her hand clutched at her chest.
Marie was admitted to Salem Hospital, north of Boston. The staff treated her COPD, a chronic lung condition that includes emphysema and chronic bronchitis.
After her worst symptoms subsided, a doctor came the next day to check on her. He told Marie her oxygen levels looked good and that she was stable and ready to be discharged.
NPR is not using Marie’s last name because she, like 1 in 9 hospitalized patients, has a history of addiction to drugs or alcohol. Disclosing a diagnosis like that can make it hard to find housing, a job and even medical care in hospitals where patients with an addiction may be shunned.
But talking to the doctor that morning, Marie felt she didn’t have a choice. She had to tell him about her other medical problem.
“He said I could be released,” Marie recalled. “And I said, ‘I got to tell you something. I’m a heroin addict. And I’m, like, starting to be in heavy withdrawal. I can’t literally move, please don’t make me go.'”
Without care, discharged patients risk overdose
At many hospitals in Massachusetts and across the country, Marie would likely have been discharged anyway, while still in the pain of withdrawal. Perhaps she would leave with a list of local detox programs where she might — or might not — find help.
But a crucial opportunity to intervene and treat at the hospital would have been lost — partly because most hospitals don’t have specialists available who know how to treat addiction, and other clinicians don’t know what to do.
Hospitals typically employ all sorts of specialists who focus on critical organs like hearts, lungs and kidneys — or who treat systemic or chronic diseases of the immune system or the brain. There are specialists for children, for mental illness, for childbirth and hospice.
But if your illness is an addiction or a condition related to drug or alcohol use, there are few hospitals where patients can see a clinician — whether that be an M.D., nurse, therapist or social worker — who specializes in addiction medicine.
Their absence among hospital personnel is particularly striking at a time when overdose deaths in the U.S. have reached record highs, and research shows patients face an increased risk of fatal overdose in the days or weeks after they are discharged from a hospital.
“They’re left on their own to figure it out, which unfortunately usually means resuming [drug] use because that’s the only way to feel better,” says Liz Tadie, a nurse practitioner certified in addiction care.
In the fall of 2020, Tadie launched a new approach at Salem Hospital, using $320,000 from a federal grant that the hospital had worked for several years to secure. Tadie put together what’s known as an “addiction consult service.”
At Salem, that team included Tadie, a patient case manager, and three recovery coaches — who draw on their experience with addiction to advocate for patients and help them navigate their treatment options.
What an addiction consult service brings to the bedside
So on that day, when Marie said, “Please don’t make me go,” her doctor didn’t tell Marie she had to leave. He called Tadie for a bedside consult.
Tadie started out the treatment by first prescribing methadone, a medication to treat opioid addiction. Although many patients do well on that drug, it didn’t help Marie, so Tadie switched her to buprenorphine, with better results. After a few more days, Marie was eventually discharged and continued taking buprenorphine to manage her addiction to opioids.
But Marie continued seeing Tadie for treatment as an outpatient and was able to turn to her for support and reassurance:
“Like, that I wasn’t going to be left alone,” Marie said. “That I wasn’t going to have to call a dealer ever again, that I could delete the number. I want to get back to my life. I just feel grateful.”
Among Salem’s clinical staff, Tadie helped spread the word about the expertise she can offer and how it can help patients. Success stories like Marie’s helped her make the case for addiction medicine — which also meant unraveling decades of misinformation, discrimination and ignorance about patients with an addiction and their treatment options.
Part of the problem, according to Tadie, is that doctors, nurses and other clinicians get very little training in the physiology of addiction and withdrawal, the medications and treatment options, and the emerging science about what works for these patients. What little training that doctors and nurses do get is often unhelpful.
“A lot of the facts are outdated,” Tadie says. “And people are training to use stigmatizing language — words like ‘addict’ and substance ‘abuse.'”
Tadie gently corrected doctors at Salem Hospital, for example, who thought they weren’t ever allowed to start patients on methadone in the hospital.
“Sometimes I would recommend a dose and somebody would give pushback,” Tadie says. But “we got to know the hospital doctors and they, over time, were like, “OK, we can trust you. We’ll follow your recommendations.”
Over time, addiction specialists help change the culture
Other members of Tadie’s team have also wrestled with finding their place in the hospital hierarchy. David Cave, one of the recovery coaches at Salem Hospital, is often the first person to speak to a patient who comes to the emergency room in withdrawal. He tries to help doctors and nurses understand what the person is going through and help navigate their care.
“I’m probably punching above my weight every time I try to talk to a clinician or doctor,” says Cave. “They don’t see letters after my name. It can be kind of tough.”
But naming addiction as a specialty, and hiring people with training in this particular disease, is shifting the culture of Salem Hospital, according to Jean Monahan-Doherty, a social worker who has referred patients to Tadie.
“There was finally some recognition across the entire institution that this was a complex medical disease that needed the attention of a specialist,” Monahan-Doherty says. “People are dying. This is a terminal illness unless it’s treated.”
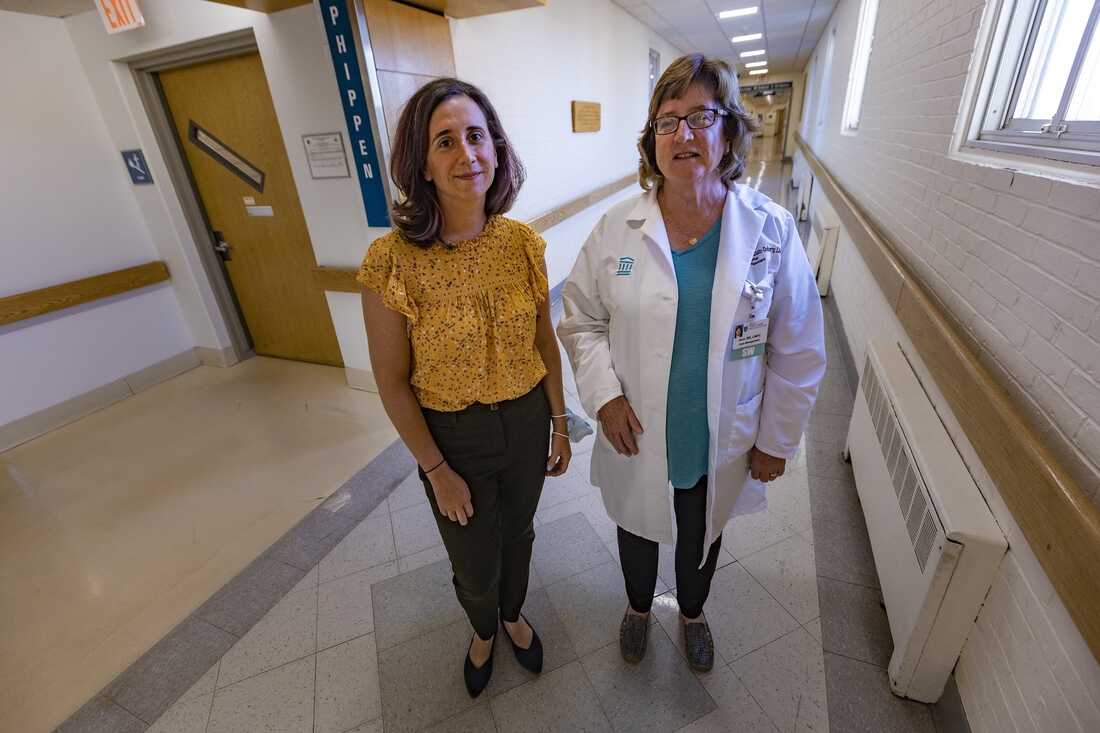
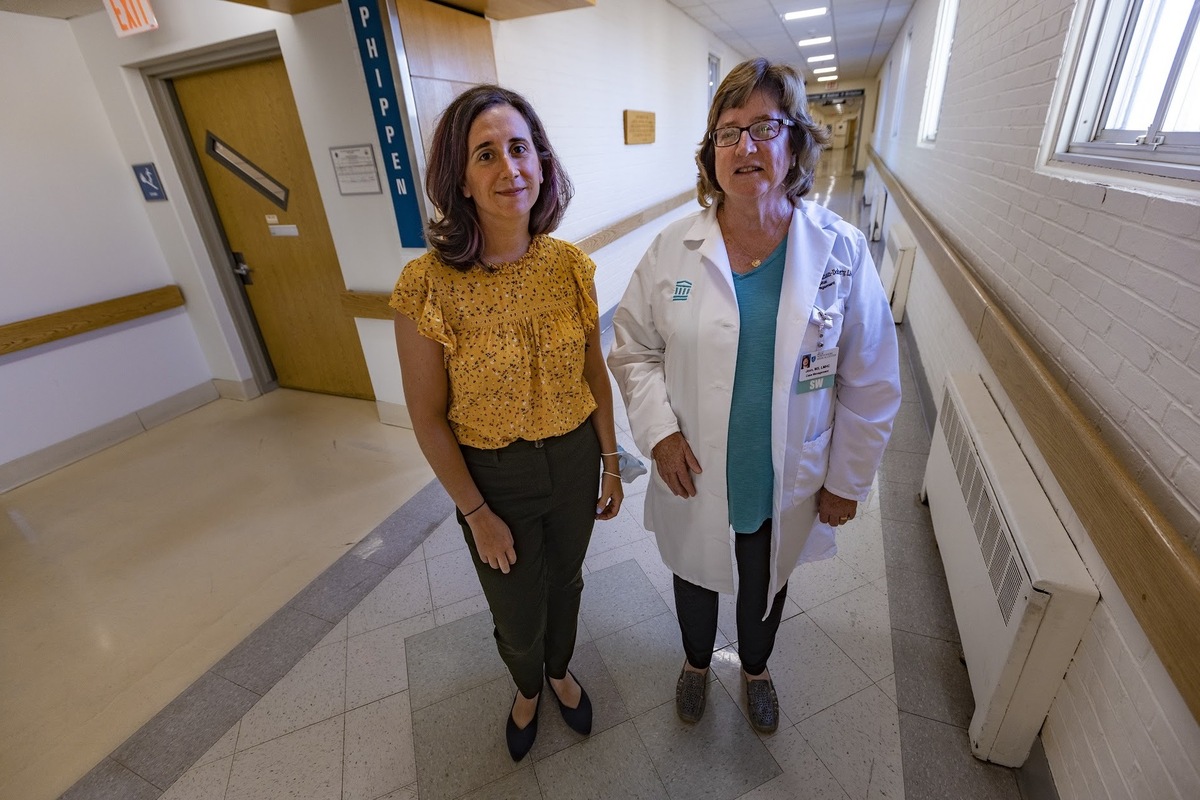
Former director of substance use disorder services at Salem Hospital Liz Tadie (left) and social worker Jean Monahan-Doherty. Tadie is moving to a new job at another hospital, but Salem Hospital leaders say they are committed to continuing the program.
Jesse Costa/WBUR
hide caption
toggle caption
Jesse Costa/WBUR
Former director of substance use disorder services at Salem Hospital Liz Tadie (left) and social worker Jean Monahan-Doherty. Tadie is moving to a new job at another hospital, but Salem Hospital leaders say they are committed to continuing the program.
Jesse Costa/WBUR
This approach to treating addiction is winning over some Salem Hospital employees — but not all.
“Some of the medical staff continue to see it as a moral issue,” Monahan-Doherty says. “Sometimes you hear an attitude of ‘Why are you putting all this effort into this patient? They’re not going to get better.’ Well, how do we know? If a patient comes in with diabetes, we don’t say, ‘OK, they’ve been taught once and it didn’t work. So we’re not going to offer them support again.'”
Despite lingering reservations among some colleagues, the demand for their services is quite high. Many days, Tadie and her team have been overwhelmed with referrals.
With federal support, states experiment to stop overdose deaths
Four other Massachusetts hospitals also added addiction specialists in the past three years and experienced similar challenges and success. The additional staff were paid for by federal funding from the HEALing Communities study. This project is paying for a wide range of strategies across several states, to determine the most effective ways to reduce drug overdose deaths. They include mobile treatment clinics, street outreach teams, naloxone trainings and distribution, rides to treatment sites, and multilingual public awareness campaigns.
“You really do provide better care for patients and you make the care environment one that people are more satisfied working in,” says Dr. Jeffrey Samet, who leads the Massachusetts portion of this research effort. Samet practices primary care at Boston Medical Center and says adding addiction specialists in hospitals is a key piece of the solution.
Dr. Todd Kerensky, president of the Massachusetts Society of Addiction Medicine, has seen patients cry when they learn he specializes in addiction and wants to treat their disease, not shame them.
“It’s gut-wrenching to know there are a lot of institutions that don’t have this service,” says Kerensky. It’s not clear how many hospitals in Massachusetts have addiction experts on staff, but Kerensky says it’s a “distinct minority.”
There are many possible reasons. It’s a new field, so finding qualified staff members with the right certifications may be a hurdle. Some hospital leaders say they’re worried about the costs of addiction treatment and fear they’ll lose money on the efforts. Some doctors report not wanting to initiate a treatment medication while the patient is still in the hospital, because they don’t know where to refer patients after they’ve been discharged, whether that be outpatient follow-up care or a residential program. To address follow-up care, Salem Hospital started what’s known as a “bridge clinic,” where patients get help transitioning to outpatient care.
Despite these worries and reservations, hospitals that don’t have an addiction specialty team need to start one, says Dr. Honora Englander, a national leader in addiction specialty programs.
“People with substance use disorder are coming to our hospitals now,” said Englander, who directs an addiction care team at Oregon Health and Science University. “We can’t wait. We have to do better, and this is the time.”
Englander says the federal government could support the creation of more addiction consult services by offering financial incentives — or penalties for hospitals that don’t embrace them. The Centers for Medicare & Medicaid Services, which has regulatory authority over most U.S. hospitals, could require that hospitals stock the medications used to treat an addiction and track outcomes for patients hospitalized with a substance use disorder, in the same way that CMS already does when it comes to readmissions for other health conditions.
At Salem Hospital, the program is still new, and some staff worry about its future. Liz Tadie is moving to a new job at another hospital, and the federal grant ended June 30. But Salem Hospital leaders say they are committed to continuing the program, and the service will continue.
Compared to the other four Massachusetts hospitals that launched addiction consult teams using the same federal grant, Salem Hospital has helped the most patients. Over a 15-month period, its team helped 448 patients begin medication to treat their opioid use disorder.
This story comes from NPR’s health reporting partnership with WBUR and KHN (Kaiser Health News).
At a certain point, it might not be easy to maintain one’s fitness past a certain age. That goal doesn’t appear to be so rigorous for bodybuilding legend and Hollywood and television icon Lou Ferrigno.
On Sept. 28, 2022, Ferrigno shared a post on his Instagram where he’s holding his shirt up in a selfie to showcase his tight abs at the age of 70. As he writes in the caption of his post, Ferrigno is “proud” to be able to stay “dedicated” and in shape after “58 years” of training and competition.
As a bodybuilder, Ferrigno competed in some intermittent capacity over the course of two decades.
The first tentpole victory of his career was a breakout win in the 1973 International Federation of Bodybuilding and Fitness (IFBB) Mr. America. That same year would see Ferrigno win the first of two straight IFBB Mr. Universe titles (1973-1974). He would later capture the 1974 IFBB Mr. International contest. Ferrigno made his Olympia debut at the 1974 Mr. Olympia, where he would finish in second to Arnold Schwarzenegger.
The following year, 1975, saw Ferrigno take home a third-place result behind Serge Nubret and the defending champion Schwarzenegger, respectively. From there, Ferrigno would not pose on an official bodybuilding stage again until he was in his early 40s during a 12th-place result at the 1992 Mr. Olympia. He would cap his career with a second-place finish in the Master’s division at the 1994 Olympia. That would be Ferrigno’s final bodybuilding competition before a formal retirement at the age of 43.
Outside of the bodybuilding and fitness sphere, some might recognize Ferrigno for his long-time famous role as Dr. Bruce Banner in CBS’s The Incredible Hulk from 1977-1982. The actor has since reprised his time as the Hulk in modern cameos in Marvel’s cinematic universe. In a further nod to his physique, Ferrigno also played the ripped Roman god Hercules in a 1983 live-action interpretation of the mythological figure. Ferrigno would play himself in a recurring part on the CBS sitcom The King of Queens and in the 2009 comedy I Love You Man alongside actors Jason Segel and Paul Rudd.
According to IMDB, Ferrigno is still staying active in Hollywood and has 70 acting credits to his name at the time of this writing. He is currently filming the movie Hermit, where he plays the eponymous character.
For a bodybuilding and Hollywood legend like Ferrigno, it seems life never stops moving at warp speed.
Featured image: @theofficiallouferrigno on Instagram
Recently, after a week in which 2,789 Americans died of COVID-19, President Joe Biden proclaimed that “the pandemic is over.” Anthony Fauci described the controversy around the proclamation as a matter of “semantics,” but the facts we are living with can speak for themselves. COVID still kills roughly as many Americans every week as died on 9/11. It is on track to kill at least 100,000 a year—triple the typical toll of the flu. Despite gross undercounting, more than 50,000 infections are being recorded every day. The CDC estimates that 19 million adults have long COVID. Things have undoubtedly improved since the peak of the crisis, but calling the pandemic “over” is like calling a fight “finished” because your opponent is punching you in the ribs instead of the face.
American leaders and pundits have been trying to call an end to the pandemic since its beginning, only to be faced with new surges or variants. This mindset not only compromises the nation’s ability to manage COVID, but also leaves it vulnerable to other outbreaks. Future pandemics aren’t hypothetical; they’re inevitable and imminent. New infectious diseases have regularly emerged throughout recent decades, and climate change is quickening the pace of such events. As rising temperatures force animals to relocate, species that have never coexisted will meet, allowing the viruses within them to find new hosts—humans included. Dealing with all of this again is a matter of when, not if.
In 2018, I wrote an article in The Atlantic warning that the U.S. was not prepared for a pandemic. That diagnosis remains unchanged; if anything, I was too optimistic. America was ranked as the world’s most prepared country in 2019—and, bafflingly, again in 2021—but accounts for 16 percent of global COVID deaths despite having just 4 percent of the global population. It spends more on medical care than any other wealthy country, but its hospitalswerenonethelessoverwhelmed. It helped create vaccines in record time, but is 67th in the world in full vaccinations. (This trend cannot solely be attributed to political division; even the most heavily vaccinated blue state—Rhode Island—still lags behind 21 nations.) America experienced the largest life-expectancy decline of any wealthy country in 2020 and, unlike its peers, continued declining in 2021. If it had fared as well as just the average peer nation, 1.1 million people who died last year—a third of all American deaths—would still be alive.
America’s superlatively poor performance cannot solely be blamed on either the Trump or Biden administrations, although both have made egregious errors. Rather, the new coronavirus exploited the country’s many failing systems: its overstuffed prisons and understaffed nursing homes; its chronically underfunded public-health system; its reliance on convoluted supply chains and a just-in-time economy; its for-profit health-care system, whose workers were already burned out; its decades-long project of unweaving social safety nets; and its legacy of racism and segregation that had already left Black and Indigenous communities and other communities of color disproportionately burdened with health problems. Even in the pre-COVID years, the U.S. was still losing about 626,000 people more than expected for a nation of its size and resources. COVID simply toppled an edifice whose foundations were already rotten.
In furiously racing to rebuild on this same foundation, America sets itself up to collapse once more. Experience is reputedly the best teacher, and yet the U.S. repeated mistakes from the early pandemic when faced with the Delta and Omicron variants. It got early global access to vaccines, and nonetheless lost almost half a million people after all adults became eligible for the shots. It has struggled to control monkeypox—a slower-spreading virus for which there is already a vaccine. Its right-wing legislators have passed laws and rulings that curtail the possibility of important public-health measures like quarantines and vaccine mandates. It has made none of the broad changes that would protect its population against future pathogens, such as better ventilation or universal paid sick leave. Its choices virtually guarantee that everything that’s happened in the past three years will happen again.
The U.S. will continue to struggle against infectious diseases in part because some of its most deeply held values are antithetical to the task of besting a virus. Since its founding, the country has prized a strain of rugged individualism that prioritizes individual freedom and valorizes self-reliance. According to this ethos, people are responsible for their own well-being, physical and moral strength are equated, social vulnerability results from personal weakness rather than policy failure, and handouts or advice from the government are unwelcome. Such ideals are disastrous when handling a pandemic, for two major reasons.
First, diseases spread. Each person’s choices inextricably affect their community, and the threat to the collective always exceeds that to the individual. The original Omicron variant, for example, posed slightly less risk to each infected person than the variants that preceded it, but spread so quickly that it inundated hospitals, greatly magnifying COVID’s societal costs. To handle such threats, collective action is necessary. Governments need policies, such as vaccine requirements or, yes, mask mandates, that protect the health of entire populations, while individuals have to consider their contribution to everyone else’s risk alongside their own personal stakes. And yet, since the spring of 2021, pundits have mocked people who continue to think this way for being irrational and overcautious, and government officials have consistently framed COVID as a matter of personal responsibility.
Second, a person’s circumstances always constrain their choices. Low-income and minority groups find it harder to avoid infections or isolate when sick because they’re more likely to live in crowded homes and hold hourly-wage jobs without paid leave or the option to work remotely. Places such as prisons and nursing homes, whose residents have little autonomy, became hot spots for the worst outbreaks. Treating a pandemic as an individualist free-for-all ignores how difficult it is for many Americans to protect themselves. It also leaves people with vulnerabilities that last across successive pathogens: The groups that suffered most during the H1N1 influenza pandemic of 2009 were the same ones that took the brunt of COVID, a decade later.
America’s individualist bent has also shaped its entire health-care system, which ties health to wealth and employment. That system is organized around treating sick people at great and wasteful expense, instead of preventing communities from falling sick in the first place. The latter is the remit of public health rather than medicine, and has long been underfunded and undervalued. Even the CDC—the nation’s top public-health agency—changed its guidelines in February to prioritize hospitalizations over cases, implicitly tolerating infections as long as hospitals are stable. But such a strategy practically ensures that emergency rooms will be overwhelmed by a fast-spreading virus; that, consequently, health-care workers will quit; and that waves of chronically ill long-haulers who are disabled by their infections will seek care and receive nothing. All of that has happened and will happen again. America’s pandemic individualism means that it’s your job to protect yourself from infection; if you get sick, your treatment may be unaffordable, and if you don’t get better, you will struggle to find help, or even anyone who believes you.
In the late 19th century, many scholars realized that epidemics were social problems, whose spread and toll are influenced by poverty, inequality, overcrowding, hazardous working conditions, poor sanitation, and political negligence. But after the advent of germ theory, this social model was displaced by a biomedical and militaristic one, in which diseases were simple battles between hosts and pathogens, playing out within individual bodies. This paradigm conveniently allowed people to ignore the social context of disease. Instead of tackling intractable social problems, scientists focused on fighting microscopic enemies with drugs, vaccines, and other products of scientific research—an approach that sat easily with America’s abiding fixation on technology as a panacea.
The allure of biomedical panaceas is still strong. For more than a year, the Biden administration and its advisers have reassured Americans that, with vaccines and antivirals, “we have the tools” to control the pandemic. These tools are indeed effective, but their efficacy is limited if people can’t access them or don’t want to, and if the government doesn’t create policies that shift that dynamic. A profoundly unequal society was always going to struggle with access: People with low incomes, food insecurity, eviction risk, and no health insurance struggled to make or attend vaccine appointments, even after shots were widely available. A profoundly mistrustful society was always going to struggle with hesitancy, made worse by political polarization and rampantly spreading misinformation. The result is that just 72 percent of Americans have completed their initial course of shots and just half have gotten the first of the boosters necessary to protect against current variants. At the same time, almost all other protections have been stripped away, and COVID funding is evaporating. And yet the White House’s recent pandemic-preparedness strategy still focuses heavily on biomedical magic bullets, paying scant attention to the social conditions that could turn those bullets into duds.
Technological solutions also tend to rise into society’s penthouses, while epidemics seep into its cracks. Cures, vaccines, and diagnostics first go to people with power, wealth, and education, who then move on, leaving the communities most affected by diseases to continue shouldering their burden. This dynamic explains why the same health inequities linger across the decades even as pathogens come and go, and why the U.S. has now normalized an appalling level of COVID death and disability. Such suffering is concentrated among elderly, immunocompromised, working-class, and minoritycommunities—groups that are underrepresented among political decision makers and the media, who get to declare the pandemic over. Even when inequities are highlighted, knowledge seems to suppress action: In one study, white Americans felt less empathy for vulnerable communities and were less supportive of safety precautions after learning about COVID’s racial disparities. This attitude is self-destructive and limits the advantage that even the most privileged Americans enjoy. Measures that would flatten social inequities, such as universal health care and better ventilation, would benefit everyone—and their absence harms everyone, too. In 2021, young white Americans died at lower rates than Black and Indigenous Americans, but still at three times the rate of their counterparts in other wealthy countries.
By failing to address its social weaknesses, the U.S. accumulates more of them. An estimated 9 million Americans have lost close loved ones to COVID; about 10 percent will likely experience prolonged grief, which the country’s meager mental-health services will struggle to address. Because of brain fog, fatigue, and other debilitating symptoms, long COVID is keeping the equivalent of 2 million to 4 million Americansout of work; between lost earnings and increased medical costs, it could cost the economy $2.6 trillion a year. The exodus of health-care workers, especially experienced veterans, has left hospitals with a shortfall of staff and know-how. Levels of trust—one of the mostimportant predictors of a country’s success at controlling COVID—have fallen, making pandemic interventions harder to deploy, while creating fertile ground in which misinformation can germinate. This is the cost of accepting the unacceptable: an even weaker foundation that the next disease will assail.
In thespring of 2020, I wrote that the pandemic would last for years, and that the U.S. would need long-term strategies to control it. But America’s leaders consistently acted as if they were fighting a skirmish rather than a siege, lifting protective measures too early, and then reenacting them too slowly. They have skirted the responsibility of articulating what it would actually look like for the pandemic to be over, which has meant that whenever citizens managed to flatten the curve, the time they bought was wasted. Endemicity was equated with inaction rather than active management. This attitude removed any incentive or will to make the sort of long-term changes that would curtail the current disaster and prevent future ones. And so America has little chance of effectively countering the inevitable pandemics of the future; it cannot even focus on the one that’s ongoing.
If change happens, it will likely occur slowly and from the ground up. In the vein of ACT UP—the extraordinarily successful activist group that changed the world’s approach to AIDS—grassroots organizations of long–haulers, grievers, immunocompromised people, and others disproportionately harmed by the pandemic have formed, creating the kind of vocal constituency that public health has long lacked.
More pandemics will happen, and the U.S. has spectacularly failed to contain the current one. But it cannot afford the luxury of nihilism. It still has time to address its bedrocks of individualism and inequality, to create a health system that effectively prevents sickness instead of merely struggling to treat it, and to enact policies that rightfully prioritize the needs of disabled and vulnerable communities. Such changes seem unrealistic given the relentless disappointments of the past three years, but substantial social progress always seems unfeasible until it is actually achieved. Normal led to this. It is not too late to fashion a better normal.
When leg day rolls around, many lifters prioritize barbell exercises like squats and Romanian deadlifts. That’s a generally reliable approach for building size and strength, but an aversion to machine exercises can make lower body workouts less effective and it can make gains harder to come by.
If lifters do incorporate machine-based movements, it’s often basic leg extensions or leg curls, and maybe a gratuitous set of calf raises. But one specific machine — a squat variation, in fact — can be the key to unlocking new muscle growth, increased strength, and improved joint health.
Credit: Vladimir Sukhachev / Shutterstock
The hack squat is very effective for building the legs and strengthening the knees and hips. It can be a staple in many routines, particularly for those looking to add muscle to their frame. It’s time to learn the ins and outs of this misunderstood machine.
How to Do the Hack Squat
The majority of commercial gyms have at least one hack squat machine, but different equipment manufacturers have slightly different designs. Some are almost completely horizontal, with the lifter lying flat on their back and moving along fixed tracks. Some machines are designed with a full support and shoulder pads on an angled track and foot platform.
Most commonly, however, a seated pad is set up on a 45-degree slant, sometimes called a “linear” or “hip sled” hack squat. An angled foot platform allows your entire lower body to run parallel to the weighted sled, with a seat designed to keep your upper body vertical. There is often a pad supporting the lower to mid-back, no upper back support, and a pair of handles on either side of the seat to hold onto.
Step 1 — Get Your Stance Right
Credit: Darryl Rose Fitness / YouTube
Take a seat and place your feet on the platform. Your lower body flexibility and mobility will influence exactly where you set your feet. The key is to be able to keep your heels flat on the platform as your knees bend fully throughout the entire range of motion.
It’s about finding the sweet spot, which is often around hip-width toward the middle of the platform. Don’t place your feet too high on the platform, too low, too narrow, or too wide — find your Goldilocks stance. What matters most is allowing your knee and ankle joints to achieve a long, pain-free range of motion.
Keep your legs slightly bent without disengaging the safety pins. Sit with your back supported on the pad. Keep your posture upright with your shoulders pulled back.
Form Tip: Try wearing a pair of shoes that add to your lower body support. Sometimes minimalist shoes can create an inadequate base and exacerbate foot issues people have with arch collapse. If it takes switching out of your bare feet or Chuck Taylors and wearing a sturdy pair of lifting shoes while performing a few sets, take the extra step to get the most out of the lift.
Step 2 — Lower Yourself into a Deep Squat
Credit: Darryl Rose Fitness / YouTube
Press through your entire foot and straighten your legs while releasing the safety. Grip the side handles tightly. Maintain good posture and don’t compromise a “proud” chest position.
Slowly lower your body by bending your knees until your upper thigh is roughly 90-degrees to your hip joint — as long as your knees can handle it without pain. Keep your feet flat on the platform and maintain contact between your hips and the pad. Pause briefly in the bottom position.
Form Tip: No matter the specific model of hack squat machine, squeeze the handles tightly throughout the exercise. Keeping a tight grip can improve upper body stability and reinforce a strong posture. (1)
Step 3 — Lift Strong to Lockout
Credit: Darryl Rose Fitness / YouTube
Without bouncing out of the bottom position, straighten your legs by applying strong and steady pressure through both feet. Don’t let your knees cave inward or bow outward.
Press hard into the platform, transferring a powerful leg drive through your hips and into the seat, as you straighten your legs and “stand” back into the top position.
Form Tip: The hack squat is ideal for accumulating mechanical tension, which is very effective for hypertrophy (muscle growth). (2) To keep the working muscles under tension, stop just shy of fully extending or straightening your legs, and keep your knee and hip joints slightly flexed (before lockout).
Hack Squat Mistakes to Avoid
Like most multi-joint movements, not paying attention to details can invite the use of sloppy form and dangerous technique. Troubleshooting this by pinpointing specific mistakes can help you stay ahead of the curve. Here’s how to prevent these follies from taking hold.
Insufficient Range of Motion
Partially bending your knees and performing shallow reps is often due to excessively heavy weight that cannot be lifted through a full range of motion. This reduces muscle activity and short-changes your results. (3)
Credit: Africa Studio / Shutterstock
A joint should be trained through its entire available active range of motion. It should also be made strong through that range. (4) There’s no reason why this shouldn’t be the case for basically every load-bearing joint in the body — that’s how you build general physical preparedness and drastically reduce injury risk.
Free weight movements like lunges or front squats involve plenty of total-body stabilizing and muscular coordination, but the hack squat machine lets you pursue a healthy, deep range of motion while loading all involved muscles and distributing stress evenly across joints.
The machine’s support pads drastically reduce the stabilizing and coordination elements, so you can and should focus solely on working through a complete range of motion.
Avoid it: Keep the weight on the lighter side to ensure a full range of motion. Aim to get your upper thigh at a 90-degree angle to your hips on every repetition. When you can do the desired set of reps with that range of motion, it’s time to progress to a heavier load.
Lifting Your Heels
Whether this comes from poor ankle mobility, general negligence, or an attempt to “target the quads” more than simple flat-footed squatting, it’s best to avoid rising onto your toes, especially when you’re learning the hack squat.
Credit: djile / Shutterstock
Lifting your heels off of the platform places all of the weight and stress onto the balls of your feet, and will result in plenty of stress also being placed on your knee joints. While some lifters’ knees may be able to handle this extreme stress, it’s still not winning the risk:reward ratio.
Avoid it: Think about elevating the toes slightly off the platform during your descent. This will emphasize your heels staying down. Think about pressing “away” with your feet like you’re about to jump backward, rather than pressing “straight down”, as if you’re about to jump up. This will help keep your full foot involved, and encourage your heels to stay planted.
Slouching with a Weak Core
It may seem like a relatively insignificant detail since the hack squat is a lower body exercise, but your upper body posture plays a role in performance. It’s just like any exercise — the more muscles the entire body can involve in bracing and tightness, the better quality the lift will be as a whole.
Credit: kristian ezcurra / Shutterstock
With the hack squat, slouching forward and not keeping an engaged core can result in you “leaking strength” for the lift, which reduces your ability to apply maximum force.
Avoid it: Begin upper body bracing with your grip strength. Hold on to those handles tightly to and tense your upper back by squeezing your shoulder blades together. Maintain that tension throughout the whole set.
Benefits of the Hack Squat
The hack squat can be a key player in your leg workout whether you’re after muscular size or raw strength and power. Just because it’s a machine doesn’t make it less effective than a barbell.
Leg Size
The hack squat removes the need for total-body stabilizing and spatial awareness, and creates a fixed path movement. This allows greater “isolation” to the lower body. While it’s still a multi-joint exercise involving the hips, knees, and ankles, the muscles above the waist are not directly targeted like they would be during back squats, for example.
Credit: Vladimir Sukhachev / Shutterstock
This makes it easier to tap into the muscles of the lower body and stimulate them for hypertrophy (muscle growth). The unique angle of the machine also allows the muscles to be put under constant tension, which further stimulates growth.
Lower Body Strength
Because the hack squat involves the quadriceps, hamstrings, and glutes, it has the potential to be loaded with relatively heavy weights. Your legs can be targeted with decreased strain on the lower back, making the hack squat an effective way to build lower body strength without the lower back wear and tear from barbell squats or deadlifts.
Knee Strengthening
It’s no secret that the knee joint is put under a fair amount of pressure when performing the hack squat, and that’s actually the reason why many lifters avoid the movement altogether. However, for healthy individuals without pre-existing knee issues, this can create beneficial stress on the connective tissues of the knee, and joint health can potentially improve in the long-term.
To make any joint stronger, just like making any muscle stronger, a lifter will have to get comfortable with a bit of discomfort. Improving joint strength requires adding (reasonable) stress to that joint, and using sound technique, appropriate loading, and progressive volume is the most effective path.
Muscles Worked by the Hack Squat
As a squat variation, the hack squat certainly targets your legs. The machine’s path and angle of resistance offer a unique training variety and stimulate the muscles slightly differently than other variations, making it a highly effective movement.
Quadriceps
The quads are the main muscle group hit by the hack squat. This is a group of four muscles on the front of the thigh that attach through one common tendon at the top of the knee. Since they have one common point of attachment, it’s difficult to isolate the quad muscles individually, but the hack squat trains them very effectively as a group.
The quadriceps’ main role is to extend the knee joint (straighten the leg), so achieving a deep knee bend is important to work the muscles through a full range of motion.
Glutes and Hamstrings
The hamstrings and glutes, the entire back half of your upper legs, are relatively less involved during the hack squat. Both muscle groups play a role in hip extension (pulling your lower body backward in line with your torso), which isn’t a significant movement pattern during the hack squat.
The glutes and hamstrings both play a small role in controlling your descent and transitioning out of the bottom position.
Hip Flexors
Your hip flexor muscles, found above your quadriceps on either side of your pelvis, are also involved in the hack squat. They work to bring your thighs closer to your torso, so they are highly activated in the lower part of the range of motion.
Because your legs are set at a fixed angle relative to your torso, your hips flexors are under constant tension because the hack squat keeps your hip joint from fully extending (stretching) throughout the movement.
Who Should Do the Hack Squat
This exercise spans a broader audience than may meet the eye. While it is a relatively specialized machine, it can be used very effectively by lifters with a variety of training goals.
Muscle-Focused Lifters
The hack squat is an effective movement for any lifter who wants to make their legs grow. It’s a staple in many bodybuilders’ quad-focused workouts because it allows the quadriceps to take the majority of training stimulus with minimal strain on the lower back or other supporting muscles.
Lifters who have a hard time isolating their quads with other movements like barbell squats, due to having longer legs, poor leverages, or mobility restrictions, may particularly benefit from the hack squat. There’s no escape from plenty of quad activation with this movement.
Lifters with Back Injuries
The hack squat can be useful for lifters with prior back injuries who want to continue hard leg training. If your spine can no longer handle squatting with a barbell on your back, the hack squat can allow you to keep loading relatively heavy weights with a big compound (multi-joint) squat variation.
Beginners
Beginners can often benefit from the added stability and predictability of the hack squat machine. The movement pattern is pre-determined, so lifters are able to use proper technique more easily. Using the hack squat in conjunction with more challenging movements (like squats and lunges) can be a great way to find results faster and build crucial training confidence.
How to Program the Hack Squat
The hack squat is most often used as a secondary exercise, performed after another compound lift like squats, deadlifts, or even split squats. This allows the hack squat to more thoroughly work the target muscles without affecting the stability requirements of free weight exercises.
Moderate Weight, Moderate Repetition
For optimal muscle-building, the best course of action is to chase reps into the double-digits. Three to five sets of 10 or more reps. Aim to accumulate relatively high training volume on this exercise — plenty of sets and reps — to maximize the hypertrophy signal.(5)
Moderate to Heavy Weight, Lower Repetition
If you decide to make the hack squat your primary movement of the workout, you can increase the weight used and lower the reps, since your central nervous system will have a little bit more in the tank when you’re completely fresh. Four to five sets of five to eight reps will let you move heavier weights while still maintaining perfect form.
Hack Squat Variations
The hack squat machine is one specific exercise, but the hack squat movement is, itself, a more general squat variation. There are several options to get the strength-building and joint health benefits if you don’t have access to a genuine hack squat machine.
Landmine Hack Squat
The landmine hack gives your ankles a more open angle to move through because your feet are flat on the ground rather than angled. That means happier knees and even more range of motion. Having the weight set in a landmine unit also allows you to make minor lateral adjustments to find the perfect groove.
Turning around and having your back against the weight plates allows you to find the perfect degree of “body lean” and the right foot position, similar to squatting with a Smith machine, without the confines of a completely fixed path. This combines to deliver a great pump, since you’re constantly using your quads to push back against the weight and maintain your body’s angle.
Barbell Hack Squat
Technically speaking, this is the original hack squat. Named after George Hackenschmidt, a European strongman from the very early 20th century, this movement is done by placing a barbell just behind your heels, squatting down, grabbing the bar, and lifting it up.
Elevating your heels with a block or weight plate changes the angle of your ankles, similar to wearing weightlifting shoes, and encourages a deep squat position. The barbell also acts as a counterbalance and allows an upright torso, which reduces lower back strain.
Reverse Hack Squat
This is a simple variation of the hack squat done on machines with full back supports and shoulder pads. By facing into the machine, you can allow your hips to move backwards, similar to a barbell back squat, which can increase hamstring and glute activity.
However, you must maintain a neutral spine. Hinging excessively at the hips and creating a more horizontal torso angle can drastically increase stress on your lower back. Some lifters may also find that their knees move forward and hit the machine’s rails, forcing them to keep their knees and lower legs at an awkward or inefficient angle.
Hack Squat Alternatives
Without a hack squat machine or effective variations, there are several effective machine-based movement to build lower body size and strength with reduced joint strain.
Leg Press
This may be the most common hack squat alternative since the two movements share many similarities. Both exercises keep your feet on a platform, which places your knees as the prime moving joint rather than your hips, and affects muscle recruitment. Both movements also require your hips to remain flexed due to your lower body’s position relative to your upper body.
The leg press may be a suitable option for people who experience too much knee stress from hack squats, since the foot platform is now moving toward your body as opposed to your body moving toward the foot platform. This subtle change can make a big difference for managing knee stress. (6)
Smith Machine Squat
The Smith machine squat is another popular and effective alternative to the hack squat (and a relatively popular alternative to barbell squatting, too).
One key benefit to the Smith machine is the ability to set your feet well in front of the bar, ensuring a vertical shin angle. Because this position does not allow your knees to move forward, there’s extremely little stress on your knee joints (which also means little joint-strengthening benefit). However, the muscular stress on the quadriceps is significantly increased.
FAQs
Should I always squat deep?
Generally, you’ll stimulate better overall results — more muscle growth, more strength, and more mobility — by working in the maximum range of motion you can achieve in the working joints. If you’re physically unable to squat extremely deep, squat to your current best depth.
With consistency and effort, your range of motion will improve right along with your muscle gains and your weights. The only time to avoid squatting deep is when you make a conscious decision to adjust the range of motion to apply a specific training method.
For example, some lifters might deliberately perform short range of motion squats to use heavier weights as a short-term overload phase, before returning to full range of motion training. That’s a far cry from accidentally loading too much weight on the bar and shaving reps high to massage your ego.
Time to Hack It
The hack squat is a movement that is for everyone and not for everyone at the same time. Rather than vilifying certain exercises based on what the pro-barbell “gym bros” say or what the functional-based “research” may purport with insufficient context, it’s better to remember that everyone isn’t built the same. Your individual mileage may vary with any exercise, and it’s up to you to apply the power of trial and error.
Hack squats can provide significant benefits when it comes to quad strengthening and muscle-building. The movement caters to both the beginning lifter looking to find his groove and the advanced lifter who’s putting the finishing touches on their lower body physique. Give the lift a fair try and discover how it works for you.
References
Gontijo, L. B., Pereira, P. D., Neves, C. D., Santos, A. P., Machado, D., & Bastos, V. H. (2012). Evaluation of strength and irradiated movement pattern resulting from trunk motions of the proprioceptive neuromuscular facilitation. Rehabilitation research and practice, 2012, 281937. https://doi.org/10.1155/2012/281937
Schoenfeld B. J. (2010). The mechanisms of muscle hypertrophy and their application to resistance training. Journal of strength and conditioning research, 24(10), 2857–2872. https://doi.org/10.1519/JSC.0b013e3181e840f3
Kubo, K., Ikebukuro, T., & Yata, H. (2019). Effects of squat training with different depths on lower limb muscle volumes. European journal of applied physiology, 119(9), 1933–1942. https://doi.org/10.1007/s00421-019-04181-y
Pallarés, JG, Hernández-Belmonte, A, Martínez-Cava, A, Vetrovsky, T, Steffl, M, Courel-Ibáñez, J. Effects of range of motion on resistance training adaptations: A systematic review and meta-analysis. Scand J Med Sci Sports. 2021; 31: 1866– 1881. https://doi.org/10.1111/sms.14006
Mangine, G. T., Hoffman, J. R., Gonzalez, A. M., Townsend, J. R., Wells, A. J., Jajtner, A. R., Beyer, K. S., Boone, C. H., Miramonti, A. A., Wang, R., LaMonica, M. B., Fukuda, D. H., Ratamess, N. A., & Stout, J. R. (2015). The effect of training volume and intensity on improvements in muscular strength and size in resistance-trained men. Physiological reports, 3(8), e12472. https://doi.org/10.14814/phy2.12472
Escamilla, R. F., Fleisig, G. S., Zheng, N., Lander, J. E., Barrentine, S. W., Andrews, J. R., Bergemann, B. W., & Moorman, C. T., 3rd (2001). Effects of technique variations on knee biomechanics during the squat and leg press. Medicine and science in sports and exercise, 33(9), 1552–1566. https://doi.org/10.1097/00005768-200109000-00020
The average heart is about the size of an adult’s fist and is made up of the atria, ventricles, valves, and several arteries and veins. A healthy heart helps in maintaining the overall well-being of the body by performing important functions like:
Pumping oxygenated blood throughout the body
Transporting hormones and other vital substances through the bloodstream to different parts of the body
Maintaining a healthy blood pressure
Sending deoxygenated blood to the lungs for oxygenation
Here are some interesting facts about the heart:
The first case of heart disease was recognized in a 3,500 years old Egyptian mummy
The risk of getting a heart attack is relatively higher on Monday
A human heart weighs less than one kilogram but manages the functioning of approximately 60,000 miles of blood vessels spread across the body
Laughing is very good for your heart as it minimizes the amount of stress and aids in boosting the immune system
The heart is a very complex organ and crucial for your survival. Thus, it is necessary to keep it healthy by exercising regularly, eating a well-balanced diet, and quitting habits that are injurious to the heart’s health.
On this World Heart Day, we emphasize the most common heart diseases in the world, causes of heart diseases, symptoms that the heart manifests when it’s unhealthy, the best foods that help in maintaining a healthy heart, and the best exercises to enhance heart health.
5 most common heart diseases
Heart diseases, also termed cardiovascular diseases (CVDs) are the leading cause of global deaths that occur due to disorders of the heart and blood vessels. According to the World Health Organization (WHO), approximately 17.9 million people died from CVDs in 2019, which is around 32% of all global deaths. Nearly 85% of deaths in this data were due to heart attack and stroke.
The heart plays a very challenging role in the process of keeping us alive. Since the organ is related to every part of the body, it is no surprise that there are several ailments related to it. In this list, we will discuss the five most common heart disease types:
Congenital heart diseases (CHDs)
CHDs are the most common birth defects that occur as a hole in the heart or maybe something more severe. The main cause of CHD is still unknown, however, 15 to 20% of cases occur due to genetic conditions.
Doctors can diagnose these problems in the baby during pregnancy, but the body may not manifest any symptoms until the baby reaches adulthood. And in some cases, the symptoms may not even occur at all. People living with CHDs face health problems, such as:
Issues with body growth and eating habits
Difficulty being physically active
Heart rhythm problems
Increased chances of heart failure
Some of the primary causes of CHD include:
Poor diet of the mother and/or excessive medication
Maternal diabetes
A habit of smoking in either of the parents
Coronary artery disease (CAD)
CAD is the most common heart disease in which the supply of blood and oxygen to the heart is obstructed as the arteries become too narrow. The condition develops when the waste products from the cells and/or cholesterol build up on the artery walls, gives rise to plaque, which can lead to a heart attack.
Maintain a healthy weight and keep blood pressure & cholesterol levels under control
Heart arrhythmia
Heart arrhythmia is a condition in which the heart starts to beat too slow or too fast due to irregular electrical impulses that coordinate heartbeats. It can occur due to excessive intake of caffeine, nicotine, alcohol, diet pills, and certain medications.
This condition is harmless in some cases and may cause minor inconveniences, but if you are suffering from any other heart illness that can exacerbate the condition, you may require immediate medical attention. These illnesses include CAD, high blood pressure, or valve disorders.
Dilated cardiomyopathy
Dilated cardiomyopathy is a life-threatening condition that mostly affects adults between the 20s and 60s. The disease starts in the left ventricle, which is the main pumping chamber of the heart, and dilates the heart muscles. Consequently, the inside of the chamber expands and the problem progresses to the right ventricle and atria.
If the treatment is delayed, the heart muscle walls weaken and won’t be able to pump the blood effectively. This can lead to shortness of breath, swelling of the ankles, feet, legs, abdomen, neck veins, and extreme tiredness.
Pulmonary stenosis
Pulmonary stenosis is a birth defect in which the pulmonary valve becomes narrowed and rigid, which obstructs the regular blood flow. In this condition, the stress on the right ventricle of the child’s heart increases as it works harder to maintain the blood flow in the pulmonary artery. To compensate for the extra stress, the right ventricle gradually thickens.
This can give rise to a condition called hypertrophy – an increase in the size of an organ due to swelling. This condition isn’t too dangerous, but it necessitates the intervention of a specialist due to the tender age of the patient.
They are high in vitamins, minerals, and antioxidants, and help manage blood pressure and promote arterial function. Vegetables like broccoli, spinach, tomatoes, bell peppers, cauliflower, beans, carrots, and beetroots are very beneficial for heart health.
Whole-grain foods are enriched with fiber which can help lower and manage the cholesterol levels in the body, which reduces the risk of heart ailments. Whole wheat, brown rice, oats, rye, barley, buckwheat, and quinoa are some of the most common and easily available whole grains foods.
Strawberries, blueberries, blackberries, and raspberries are excellent sources of antioxidants like anthocyanins, which protect the body from oxidative stress and inflammation, which reduces the risk of heart ailments.
Walnuts are enriched with fiber and micronutrients such as magnesium, copper, and manganese which help in managing blood pressure, decrease oxidative stress, reduce inflammation, and lower cholesterol levels. These nutritious benefits of walnuts help promote heart health.
Garlic consist of a compound called allicin which has therapeutic medicinal properties that help reduce blood pressure and cholesterol levels. Regular consumption of garlic also decreases the chances of blood clot formation and promotes heart health.
It may sound a bit hard to believe, but brisk walking can help in improving the condition of the heart, all you need is a pair of good shoes. It increases the rate of blood flowing to the heart and is also easier on the joints (especially beneficial for those suffering from joint ailments) as compared to any other exercise.
Weight training helps in building muscles of the body, which increases blood flow and improves heart health.
Swimming is a proven full-body exercise that improves body tone, increases blood circulation, and promotes heart health.
Yoga is one of the best ways to improve heart health and promote overall well-being. Yoga helps strengthen your bones and tone your muscles, which increases blood circulation and manages blood pressure, blood sugar levels, and cholesterol levels.
Core workouts like plank and pilates help increase the strength of your core muscles and provide balance to the body. A strong core promotes your overall health and increases blood circulation which improves heart health.
Final thoughts
The heart is one of the most complex organs of the body which helps you stay alive and kicking. It functions 24/7 and ensures continuous blood circulation to every part of the body. If the functioning of the heart is obstructed, its impact can be quite severe on your overall well-being.
To ensure that your heart health is not compromised, it’s highly recommended to get diagnosed at regular intervals to ascertain your correct health condition. Take measures to avoid the aforesaid causes of heart ailments, and if you experience any symptoms, seek medical attention immediately.
Pfizer completes ResApp purchase for over $115 million
Biopharmaceutical giant Pfizer has finalised its acquisition of ASX-listed digital health startup ResApp for A$179 million ($116 million), according to the University of Queensland.
Brisbane-based ResApp has developed a mobile app that analyses cough sounds and diagnoses respiratory diseases, including asthma, pneumonia, bronchiolitis, croup and chronic obstructive pulmonary disease. The company also recently demonstrated the capability of its app to diagnose COVID-19.
Approved for use in Australia and Europe, ResAppDx can be integrated with telehealth platforms, emergency departments, and primary care settings.
New NHMRC-backed centre to apply AI in breast cancer risk classification
A risk-based approach using AI will be applied to a new breast cancer screening centre launched at the University of Melbourne.
Supported by the National Health and Medical Research Council (NHMRC), Australia’s main statutory authority for medical research, the My Breast Cancer RISK Centre (MyBRISK) will use AI to analyse millions of mammograms to identify “more powerful mammogram-based risk factors.”
These automated measures, combined with family history, lifestyle and gene tests, will enable testing to better classify women of all ages in terms of their breast cancer risk, the university said in a media release.
As present breast cancer risk assessment tools are said to be “cumbersome and lack precision,” this new NHMRC Centre for Research Excellence aims to “create pathways for more effective personalised screening.”
MyBRISK is a collaboration between the University of Melbourne, Melbourne’s St Vincent’s Hospital, Monash University, University of Western Australia, Queensland University of Technology and Cancer Council Victoria.
Digital tool reduces medication errors in children’s hospitals: research
New research in Sydney has demonstrated how the use of an electronic medication management system (eMeds) can help lower medication errors in children’s hospitals.
Conducted by Macquarie University, Sydney Children’s Hospital and eHealth NSW, the study involved the review of more than 43,000 medication orders for about 8,000 paediatric patients.
eMeds, which is now used in 200 hospitals across New South Wales to prescribe, dispense, and provide medications to patients, was developed by eHealth NSW. The technology also helps monitor interactions and doses and provides safety alerts to avoid errors.
Townsville University Hospital implements Dell’s data storage solutions
Townsville University Hospital (TUH), a tertiary referral hospital in northern Queensland, has deployed data storage solutions from Dell Technologies to enhance information sharing and care quality.
According to a press release, the hospital has adopted Dell PowerStore, a single storage platform that provides block-based storage and a centralised data lake. It has become the foundation of its ward management and patient flow reporting systems, resulting in “significant growth” in clinical media and has enabled staff to perform near real-time reporting instead of batch processing.
TUH also implemented Dell PowerScale, which provides a single repository for unstructured data.
“Together, the new storage solutions provide TUH with additional performance, improved redundancy, scalability and flexibility,” Dell said in a statement.
Singapore clears VUNO’s AI software for fundus analysis
South Korean medical AI firm VUNO has recently obtained a medical device certification from Singapore’s Health Sciences Authority for its AI-based fundus analysis software.
The VUNO Med-Fundus AI analyses images of the fundus, which is the back part of the eye, to provide findings necessary for the diagnosis of retinal diseases. It can detect the location of lesions indicative of diseases, such as diabetic retinopathy, macular disease and glaucoma, within seconds.
Through this certification, VUNO can tap into the growing medical devices market in Singapore, which is projected to reach $1 billion in value in 2024, growing at an 8.7% CAGR from 2019.
Taiwan-based Point Robotics gets 510(k) for its surgical robot system
Point Robotics, maker of surgical robots in Taiwan, has received the US Food and Drug Administration’s 510(k) clearance for its integrated robotic-assisted surgical system for spinal fusion surgeries.
The POINT Kinguide Robotic-Assisted Surgical System combines image-guided navigation and a hand-held drilling feature to streamline procedural tasks with precision, stability, and reproducibility of robot motion.
What sets it apart from similar systems, according to the company, is the parallel manipulator mechanism that enables it to expand indications for more complicated herniated disc decompression surgery.
Following the US clearance, Point Robotics is preparing for CE marking in Europe and registration in China, expanding its presence in international markets.
“We aim to promote availability and affordability of robot’s adoption for spinal surgery unaddressed by today’s technology to treat more patients who contracted a spectrum of spinal diseases,” said CEO SC Juang.
Mental health startup Lissun receives $1M in pre-seed funding
Indian mental health platform Lissun has raised $1 million in a pre-seed funding round led by IvyCap Ventures. The round was also participated by We Founder Circle, Supermorpheous and other marquee angel investors.
The startup employs a unique “B2H2C” approach – it reaches consumers through its partnerships with healthcare institutions – in offering its full-stack mental health solution. It has tie-ups with over 70 healthcare organisations in 17 cities in India.
Based on a press statement, Lissun’s technology is applied to high-stress use cases in six healthcare categories, such as infertility, rehabilitation, nephrology, and oncology, among others. “The very fact that mental and emotional issues can be an underlying problem in many medical cases is what we have identified and are working on proactively,” explained co-founder Dr Krishna Veer Singh.
Through its fresh investment, Lissun aims to strengthen its technology’s backbone and further develop it to provide a seamless user experience. Moreover, it plans to expand to 25 cities, as well as cover five more therapeutic categories.
India to repurpose COVID-19 apps
The Indian government plans to repurpose its two main mobile applications for tracking COVID-19 cases in the country.
A news report cited Dr Ram Sewak Sharma, CEO of the National Health Authority, as saying that they plan to reuse the contact tracing app Aarogya Setu as a national health app while the Covid Vaccine Intelligent Network (CoWIN) platform will be repurposed for the national immunisation programme and a health management information system for small doctors.