Oct. 12, 2022 – About 1 in 20 people with long COVID continue to live with symptoms at 18 months, and another 42% reported only some improvement in their health and wellbeing in the same time frame, a large study out of Scotland found.
Multiple studies are evaluating people with long COVID in the hopes of figuring out why some people experience debilitating symptoms long after their primary infection ends and others either do not or recover more quickly.
This current study is notable for its large size – 96,238 people. Researchers checked in with participants at 6, 12 and 18 months, and included a group of people never infected with the coronavirus to help investigators make a stronger case.
“A lot of the symptoms of long COVID are non-specific and therefore can occur in people never infected,” says senior study author Jill P. Pell, head of the School of Health and Wellbeing at the University of Glasgow in Scotland.
Ruling Out Coincidence
This study shows that people experienced a a wide range of symptoms after becoming infected with COVID-19 at a significantly higher rate than those who were never infected, “thereby confirming that they were genuinely associated with COVID and not merely a coincidence,” she says.
Among 21,525 people who had COVID-19 and had symptoms, tiredness, headache and muscle aches or muscle weakness were the most common ongoing symptoms.
Loss of smell was almost 9 times more likely in this group compared to the never infected group in one analysis where researchers controlled for other possible factors. The risk for loss of taste was almost 6 times greater, followed by risk of breathlessness at 3 times higher.
Long COVID risk was highest after a severe original infection and among older people, women, Black and South Asian populations, people with socioeconomic disadvantages and those with more than one underlying health condition.
Adding up the 6% with no recovery after 18 months and 42% with partial recovery means that between 6 and 18 months following symptomatic coronavirus infection, almost half of those infected still experience persistent symptoms.
Vaccination Validated
On the plus side, people vaccinated against COVID-19 before getting infected had a lower risk for some persistent symptoms. In addition, Pell and colleagues found no evidence that people who experienced asymptomatic infection were likely to experience long COVID symptoms or challenges with activities of daily living.
“Unfortunately, these long COVID symptoms are not getting better as the cases of COVID get milder,” says Thomas Gut, DO, Medical Director for the Post COVID recovery program at Staten Island University Hospital in New York City. “Quite the opposite – this infection has become so common in a community because it’s so mild and spreading so rapidly that we’re seeing more long COVID symptoms than ever before.”
Although most patients he sees with long COVID resolve their symptoms within 3 to 6 months, “We do see some patients who require short-term disability because their symptoms continue past 6 months and out to 2 years,” says Gut, who is also , hospitalist at Staten Island University Hospital / Northwell Health.
Patients with fatigue and neurocognitive symptoms “have a very tough time going back to work. Short-term disability gives them the time and finances to pursue specialty care with cardiology, pulmonary and neurocognitive testing,” he says.
Support the Whole Person
The burden of living with long COVID goes beyond the persistent symptoms. “Long COVID can have wide-ranging impacts — not only on health but also quality of life and activities of daily living [including] work, mobility, self-care and more,” Pell says. “So, people with long-COVID need support relevant to their individual needs and this may extend beyond the health care sector, for example including social services, school or workplace.”
Still, Lisa Penziner, RN, Founder of the COVID Long Haulers Support Group in Westchester and Long Island, NY, says while people with the most severe cases of COVID-19 tended to have the worst long-COVID symptoms, they’re not the only ones.
“We saw many post-COVID members who had mild cases and their long-haul symptoms were worse weeks later than the virus itself,” says Penziner.
Penziner estimates that 80% to 90% of her support group members recover within 6 months. “However, there are others who were experiencing symptoms for much longer.”
Respiratory treatment, physical therapy and other follow-up doctor visits are common after 6 months, for example.
“Additionally, there is a mental health component to recovery as well, meaning that the patient must learn to live while experiencing lingering, long-haul COVID symptoms in work and daily life,” says Penziner, who is also director of special projects at North Westchester Restorative Therapy & Nursing.
In addition to ongoing medical care, people with long COVID need understanding, Penziner says.
“While long-haul symptoms do not happen to everyone, it is proven that many do experience long-haul symptoms, and the support of the community in understanding is important.”
Limitations of the Study
Pell and colleagues note some strengths and weaknesses to their study. For example, “as a general population study, our findings provide a better indication of the overall risk and burden of long-COVID than hospitalized cohorts,” they note.
Also, the Scottish population is 96% white, so other long-COVID studies with more diverse participants are warranted.
Another potential weakness is the response rate of 16% among those invited to participate in the study, which Pell and colleagues addressed: “Our cohort included a large sample (33,281) of people previously infected and the response rate of 16% overall and 20% among people who had symptomatic infection was consistent with previous studies that have used SMS text invitations as the sole method of recruitment.”
“We tell patients this should last 3 to 6 months, but some patients have longer recovery periods,” Gut says. “We’re here for them. We have a lot of services available to help get them through the recovery process, and we have a lot of options to help support them.”
“What we found most helpful is when there is peer-to-peer support, reaffirming to the member that they are not alone in the long-haul battle, which has been a major benefit of the support group,” Penziner says.
If you or someone you know is experiencing long COVID and could benefit from peer support, Penziner can be contacted at [email protected]
The physical effects of overactive bladder are obvious. But the emotional impact isn’t talked about as much. You might avoid going on road trips with friends, playing sports, or visiting your grandchildren because you’re self-conscious about leaking or having to stop a lot to use the restroom.
“People start to live their lives around management of their bladder,” says Aqsa Khan, MD, a urologist at the Mayo Clinic in Phoenix, AZ.
Social Challenges
Even at home, OAB can make the simplest social interactions stressful. Khan says one of her patients, a 50-year-old woman, described having a nice chat with her neighbor in the yard when she suddenly started to pee in the middle of her conversation. To cover it up, she turned the garden hose onto herself.
The loss of control, Khan says, can be devastating. “It’s losing something that really defines you as a social being,” she says. “It makes you feel infantilized, in a way. It takes you back to wearing diapers.”
Intimacy
OAB can also impact intimacy. You might avoid sexual activity because you’re worried about leaking. This can lead to bigger relationship issues. If your partner doesn’t know what’s wrong, they may think it has something to do with them. Try your best to open up and trust your partner to be supportive.
Intimacy challenges are tough enough for couples who have been together for decades. They can be even more overwhelming when you’re in the dating game. “[OAB] can be a huge elephant in the room when starting up those more intimate relationships,” says A. Lenore Ackerman, MD, PhD. She’s the research director for UCLA Health’s Division of Female Pelvic Medicine and Reconstructive Surgery.
Sleep Trouble and Depression
You might wake up four times a night but go right back to sleep each time. Others may only get up twice a night. But they have so much trouble getting back to sleep each time that it has a huge effect on their quality of life. “It’s torture,” Khan says.
That’s because when you don’t get enough rest, your body doesn’t get the chance to recuperate. This could lead to other issues, including problems with brain function. There is a strong link between OAB and depression, Ackerman says, and poor sleep is a key factor. “Sleep is really centrally important to all of it,” she says.
Stress and Tension
The anxiety surrounding OAB can also make your physical symptoms worse. Just as you might clench your jaw without realizing it, people with OAB often clench their pelvic floor muscles, says Veronica Asence, DPT. She’s a physical therapist at Lahey Hospital & Medical Center in Burlington, MA, who specializes in pelvic health.
“Your pelvic floor is always active: supporting your pelvis, holding up your organs,” she says. “If we’re clenching our pelvic floor muscles in relation to the urge [to pee] and the anxiety surrounding that urge, it’s like we’re constantly tucking our tail.”
This nonstop squeezing can wear them out. So much so they lose control when you need them the most. You could see a big change in your symptoms just by working on ways to ease your anxiety and the pelvic floor tension that comes with it.
Fighting the Stigma
If you’re older, you might think urinary issues are a normal part of aging. (They’re not.) But if you’re young, OAB can carry an additional level of shame and self-blame. You might wonder how this could be happening or what’s “wrong” with you.
Shame can be a major block in asking for help, but OAB is more common than you think. “Talk to your friends,” Ackerman says. “Odds are some of them have it, too.” In fact, Ackerman says the first thing she does when meeting a new patient is tell them about her own urinary problems.
By talking about it more, others with OAB will likely feel more comfortable looking for long-term treatments instead of just managing symptoms with pads, backup underwear, catheters, and other items. They can be a great way to take back control. For instance, new products are often designed with light, flattering fabrics that secretly hold lots of fluids. But they sometimes stop people from getting professional help, Ackerman says.
“You don’t have to deal with this alone,” Ackerman says. “This happens to a lot of us, and there’s treatment, and we want to get you treatment.”
Talk to Your Doctor
“Physicians get into this line of work because they want to help patients,” says Sevann Helo, MD, a Mayo Clinic urologist in Rochester, MN. “We can’t improve something we don’t know is a problem.”
If your doctor doesn’t know how to treat OAB, they should refer you to someone who can. With help, you can take control. “It doesn’t matter if you’re 28 years old or 88 years old,” Asence says. “Your bladder can be retrained at any point in your lifetime.” The key, she adds, is to be persistent and take care of your whole self. “The bladder’s personality is a lot like a toddler: it does best with structure, discipline, and a healthy environment.”
WEDNESDAY, Oct. 12, 2022 (HealthDay News) — Celebrity Khloe Kardashian announced Tuesday that she had survived a second bout of skin cancer, this time on her face.
Kardashian said her “incredibly rare” tumor was removed by Beverly Hills surgeon Dr. Garth Fisher after the reality TV star noticed a bump that wouldn’t go away.
“I decided to get it biopsied 7 months after realizing it was not budging,” Kardashian, 38, wrote in an Instagram post.
Kardashian had initially thought the bump was a pimple, but later was seen by multiple doctors who told her the tumor was “incredibly rare for someone [her] age.”
She was told to have surgery immediately after the biopsy results were returned.
“All my margins appear clear and now we are onto the healing process,” Kardashian wrote over a picture of her face with a bandage. “You’ll continue to see my bandages and when I’m allowed, you’ll probably see a scar (and an indentation in my cheek from the tumor being removed).”
Kardashian had been wearing a bandage on her face for a few weeks.
In her post she also revealed that this was the second time she had skin cancer.
“At 19-years-old, I had melanoma on my back, and I had a surgery to remove that as well,” Kardashian said. “I am someone who wears sunscreen every single day, religiously so no one is exempt from these things. Please take this seriously and do regular self-exams as well as your annual checkups.”
Kardashian also shared recent videos and photos of her wearing the bandage in public, thanking her dermatologists, surgeon and also her makeup artist for “dealing with” the face bandages.
Kardashian said that she was “lucky and all I have is a scar to tell a story with. I hope you enjoy how fabulous I’m making these face bandages look.”
More information
The U.S. Centers for Disease Control and Prevention has more on skin cancer.
Oct. 12, 2022 — When 16-year-old Jake Gallagherdied of a heart attack while playing video games, the U.K. teen’s death made international headlines. Many reports called the 2013 case a rare isolated incident, noting the teen had an underlying heart condition that put him at risk.
But new research suggests such cases are more common than you might think.
Australian scientists who reviewed nearly 70 studies and reports on cardiovascular risks from electronic gaming identified 22 children and teens who lost consciousness while playing video games and experienced heart rhythm problems and other cardiac complications.
Nineteen of the mostly male gamers, aged 7 to 16, experienced serious irregular heartbeats known as ventricular arrhythmia. Six had heart attacks, and four died suddenly. The researchers also found only 7 of the 22 had received a prior diagnosis of arrhythmia or other heart problems.
“Video games may represent a serious risk to some children with arrhythmic conditions; they might be lethal in patients with predisposing, but often previously unrecognized arrhythmic conditions,” notes lead investigator Claire M. Lawley, MBBS, PhD, with The Heart Centre for Children in Sydney, Australia, in a statement. “Children who suddenly lose consciousness while electronic gaming should be assessed by a heart specialist as this could be the first sign of a serious heart problem.”
Such cases are rare, says Christian Turner, MBBS, a co-author of the report, published in the journal Heart Rhythm. Even so, the findings suggest parents monitor their children for signs of stress while gaming — such as sudden fainting or blacking out during periods of high excitement — that might signal an underlying heart condition that could put their lives in danger.
“The population at risk is exceptionally small,” he says. “Children playing games electronically would be at no greater risk than playing school sports or being physically active. For a parent, if their child has a new blackout, faint, collapse or seizure, they should be checked out by their local or family doctor. The family’s doctor will then determine if further tests are necessary.”
In an editorial accompanying the new report, Daniel Sohinki, MD, with the Department of Cardiology at Augusta University in Georgia, argues that the study’s findings suggest screening programs — similar to what’s recommended for collegiate sports — aimed at identifying underlying cardiac issues “should encompass athletes being considered for participation in eSports.”
Sohinki says what’s needed is a better understanding of how stress — mental or physical — stimulates the cardiovascular system in ways that can be dangerous to gamers and traditional sports athletes alike. The same might also be said of other highly stressful activities, such as watching horror films or exciting competitive sporting events that get your heart beating faster.
“What it comes down to is what kind of stress stimulates the cardiovascular system,” he says. “Whether that’s mental excitement or physical exertion, it’s something that increases your heart rate and increases the stimulated input to the cardiovascular system … that’s the common underlying theme between aerobic exercise and competitive video games.”
He notes that new findings should prompt a rethinking of conventional belief that video games are safer for kids with underlying heart problems than traditional sports, such as basketball, soccer, and hockey, that can put young athletes at risk for sudden cardiac death.
“I think in the past, there’s been a thought that if there’s a child who we believe is at risk for arrhythmia or some sort of cardiovascular complication from aerobic exercise, then maybe some sort of sedentary activity, like playing a video game, would be safer for them,” he says. “But what this paper argues is that if you have a child whom you believe to be at risk for a cardiac event for whatever reason, you can’t necessarily be assured that a competitive video game is going to be a safer activity for them.”
The Australian investigators who conducted the new review based their conclusions on dozens of studies and reports on children who experienced sudden loss of consciousness while playing video games and were determined to have underlying heart conditions.
Among the researchers’ findings:
Of the 22 cases identified, multiplayer war gaming was the most frequent trigger.
19 males (86%) were identified as having experienced suspected or proven ventricular arrhythmia during electronic gaming.
Six (27%) experienced cardiac arrest and four (18%) died suddenly.
Underlying heart conditions were known in just seven (31%) patients beforehand, but confirmed in 12 (54%) afterward.
The most common underlying conditions were heart rhythm disorders known as CPVD (catecholaminergic polymorphic ventricular tachycardia) and LQTS (congenital long QT syndrome).
The research team also found a high incidence of genetic variants (63%) among the gamers, which has significant implications for their families. In some cases, the investigation of a child who lost consciousness during video gaming led to other family members being diagnosed with an important familial heart rhythm problem.
Turner says he believes the researchers’ findings, while troubling, shouldn’t lead to calls for widespread screening of all children — with echocardiograms, stress tests, or other procedures — before clearing them to play video games.
“We, in Sydney, Australia, feel the potential harms of screening all children for such a rare condition outweigh the potential benefits,” he says. “Screening would entail performing an exercise stress test on every child in the community and is certainly not practical in the real world. The medical community is already well aware that syncope [loss of consciousness] during sport should be investigated. Our findings in this report suggest that syncope during electronic gaming should be similarly investigated.”
But Sohinki argues that any child who has had symptoms of a potential heart condition should at least get a standard physical exam and be evaluated for any symptoms that might suggest video gaming could pose a potential risk. These recommendations are in line with guidelines of the National College Athletic Association (NCAA) for sports athletes, which estimates sudden cardiac death strikes between 1 in 40,000 and 1 in 80,000 players each year.
“For the NCAA, the minimum is a comprehensive medical history and physical examination that’s aimed at identifying either cardiac symptoms or a personal or family history of cardiovascular disease,” he notes. “That’s recommended for all NCAA athletes. So I think there’s a strong argument to be made that … that should be extended to any person who is going to participate competitively in a video game. I think you could justify a history and physical examination as being is a cost-effective intervention. I would support that.”
For Sohinki, who has a young son and is a gamer himself, the issue is both a personal and professional concern. He practices what he preaches.
“I have a 3-year-old and he’s watched me play video games and asked to play games as well,” he says. “I also have a [heart] valve condition that is heritable, so he’s already had an echocardiogram screening. But if he didn’t have any symptoms or a known history of cardiovascular disease, I’m not sure I would have anything more than a medical history and physical screening before letting him play video games.”
Oct. 12, 2022 – Ever since his mid-30s, Greg lived in a nursing home. An assault 6 years earlier left him barely conscious, unable to talk or eat. Two years of rehab did little to help him. Most people in Greg’s condition would have remained nonverbal and separated from the world for the rest of their lives. But at age 38, Greg received a brain implant through a clinical trial.
“People who are in the minimally conscious state have intact brain circuitry, but those circuits are under-activated,” explains Joseph Fins, MD, chief of the Division of Medical Ethics at Weill Cornell Medicine in New York City. Delivering electrical impulses to affected regions can revive those circuits, restoring lost or weakened function.
The researchers switched Greg’s device off and on every 30 days for 6 months, observing how the electrical stimulation (or lack thereof) altered his abilities. They saw remarkable things.
“With the deep brain stimulator, he was able to say six- or-seven-word sentences, the first 16 words of the Pledge of Allegiance. Tell his mother he loved her. Go shopping at Old Navy and voice a preference for the kind of clothing his mother was buying,” recalls Fins, who shared Greg’s journey in his book, Rights Come to Mind: Brain Injury, Ethics and the Struggle for Consciousness.
After 6 years of silence, Greg regained his voice.
Yet success stories like his aren’t without controversy, as the technology has raised many ethical questions: Can a minimally conscious person consent to brain surgery? What happens to the people being studied when clinical trials are over? How can people’s neural data be responsibly used – and protected?
“I think that motto, ‘Move fast and break things,’ is a really bad approach,” says Veljko Dubljevic, PhD, an associate professor of science, technology, and society at North Carolina State University. He’s referring to the unofficial tagline of Silicon Valley, the headquarters for Elon Musk’s neurotechnology company, Neuralink.
Neuralink was founded in 2016, nearly a decade after the study about Greg’s brain implant was published. Yet it has been Musk’s company that has most visibly thrust neurotechnology into public consciousness, owing somewhat to its founder’s often overstated promises. (In 2019, Musk claimed his brain-computer interface would be implanted in humans in 2020. He has since moved that target to 2022.) Musk has called his device “a Fitbit in your skull,” though it’s officially named the “Link.”
Brain-computer interfaces, or BCIs, are already implanted in 36 people around the world, according to Blackrock, a leading maker of these devices. What makes Neuralink different is its ambitious goal to implant over 1,000 thinner-than-hair electrodes. If the Link works as intended – by monitoring a person’s brain activity and commanding a computer to do what they want – people with brain disorders, like quadriplegia, could regain a lot of independence.
The History Behind Brain Implants
BCIs – brain implants that communicate with an external device, typically a computer – are often framed as a science-fiction dream that geniuses like Musk are making a reality. But they’re deeply indebted to a technology that’s been used for decades: deep brain stimulation (DBS). In 1948, a neurosurgeon at Columbia University implanted an electrode into the brain of a woman diagnosed with depression and anorexia. The patient improved – until the wire broke a few weeks later. Still, the stage was set for longer-term neuromodulation.
It would be movement disorders, not depression, that ultimately catapulted DBS into the medical mainstream. In the late 1980s, French researchers published a study suggesting the devices could improve essential tremor and the tremor associated with Parkinson’s. The FDA approved DBS for essential tremor in 1997; approval for Parkinson’s followed in 2002. DBS is now the most common surgical treatment for Parkinson’s disease.
Since then, deep brain stimulation has been used, often experimentally, to treat a variety of conditions, ranging from obsessive-compulsive disorder to Tourette’s to addiction. The advancements are staggering: Newer closed-loop devices can directly respond to the brain’s activity, detecting, for example, when a seizure in someone with epilepsy is about to happen, then sending an electrical impulse to stop it.
In clinical trials, BCIs have helped people with paralysis move prosthetic limbs. Implanted electrodes enabled a blind woman to decipher lines, shapes, and letters. In July, Synchron – widely considered Neuralink’s chief competitor – implanted its Stentrode device into its first human subject in the U.S. This launched an unprecedented FDA-approved trial and puts Synchron ahead of Neuralink (which is still in the animal-testing phase). Australian research has already shown that people with Lou Gehrig’s disease (also called amyotrophic lateral sclerosis, or ALS) can shop and bank online using the Stentrode.
With breakthroughs like these, it’s hard to envision any downsides to brain implants. But neuroethicists warn that if we don’t act proactively – if companies fail to build ethical concerns into the very fabric of neurotechnology – there could be serious downstream consequences.
The Ethics of Safety and Durability
It’s tempting to dismiss these concerns as premature. But neurotechnology has already gained a firm foothold, with deep brain stimulators implanted in 200,000 people worldwide. And it’s still not clear who is responsible for the care of those who received the devices from clinical trials.
Even if recipients report benefits, that could change over time as the brain encapsulates the implant in glial tissue. This “scarification” interferes with the electrical signal, says Dubljevic, reducing the implant’s ability to communicate. But removing the device could pose a significant risk, such as bleeding in the brain. Although cutting-edge designs aim to resolve this – the Stentrode, for example, is inserted into a blood vessel, rather than through open brain surgery – many devices are still implanted, probe-like, deep into the brain.
Although device removal is usually offered at the end of studies, the cost is often not covered as part of the trial. Researchers typically ask the individual’s insurance to pay for the procedure, according to a study in the journal Neuron. But insurers have no obligation to remove a brain implant without a medically necessary reason. A patient’s dislike for the device generally isn’t sufficient.
Acceptance among recipients is hardly uniform. Patient interviews suggest these devices can alter identity, making people feel less like themselves, especially if they’re already prone to poor self-image.
“Some feel like they’re controlled by the device,” says Dubljevic, obligated to obey the implant’s warnings; for example, if a seizure may be imminent, being forced not to take a walk or go about their day normally.
“The more common thing is that they feel like they have more control and greater sense of self,” says Paul Ford, PhD, director of the NeuroEthics Program at the Cleveland Clinic. But even those who like and want to keep their devices may find a dearth of post-trial support – especially if the implant wasn’t statistically proven to be helpful.
Eventually, when the device’s battery dies, the person will need a surgery to replace it.
“Who’s gonna pay for that? It’s not part of the clinical trial,” Fins says. “This is kind of like giving people Teslas and not having charging stations where they’re going.”
As neurotechnology advances, it’s critical that health care systems invest in the infrastructure to maintain brain implants – in much the same way that someone with a pacemaker can walk into any hospital and have a cardiologist adjust their device, Fins says.
“If we’re serious about developing this technology, we should be serious about our responsibilities longitudinally to these participants.”
The Ethics of Privacy
It’s not just the medical aspects of brain implants that raise concerns, but also the glut of personal data they record. Dubljevic compares neural data now to blood samples 50 years ago, before scientists could extract genetic information. Fast-forward to today, when those same vitals can easily be linked to individuals.
“Technology may progress so that more personal information can be gleaned from recordings of brain data,” he says. “It’s currently not mind-reading in any way, shape, or form. But it may become mind-reading in something like 20 or 30 years.”
That term – mind-reading – is thrown around a lot in this field.
“It’s kind of the science-fiction version of where the technology is today,” says Fins. (Brain implants are not currently able to read minds.)
But as device signals become clearer, data will become more precise. Eventually, says Dubljevic, scientists may be able to figure out attitudes or psychological states.
“Someone could be labeled as less attentive or less intelligent” based on neural patterns, he says.
Brain data could also expose unknown medical conditions – for example, a history of stroke – that may be used to raise an individual’s insurance premiums or deny coverage altogether. Hackers could potentially seize control of brain implants, shutting them off or sending rogue signals to the user’s brain.
Some researchers, including Fins, say that storing brain data is no riskier than keeping medical records on your phone.
“It’s about cybersecurity writ large,“ he says.
But others see brain data as uniquely personal.
“These are the only data that reveal a person’s mental processes,” argues a report from UNESCO’s International Bioethics Committee (IBC). “If the assumption is that ‘I am defined by my brain,’ then neural data may be considered as the origin of the self and require special definition and protection.”
“The brain is such a key part of who we are – what makes us us,” says Laura Cabrera, PhD, the chair of neuroethics at Penn State University. “Who owns the data? Is it the medical system? Is it you, as a patient or user? I think that hasn’t really been resolved.”
Many of the measures put in place to regulate what Google or Facebook gathers and shares could also be applied to brain data. Some insist that the industry default should be to keep neural data private, rather than requiring people to opt out of sharing. But Dubljevic, takes a more nuanced view, since the sharing of raw data among researchers is essential for technological advancement and accountability.
What’s clear is that forestalling research isn’t the solution – transparency is. As part of the consent process, patients should be told where their data is being stored, for how long, and for what purpose, says Cabrera. In 2008, the U.S. passed a law prohibiting discrimination in health care coverage and employment based on genetic information. This could serve as a helpful precedent, she says.
The Legal Question
Around the globe, legislators are studying the question of neural data. A few years ago, a visit from a Columbia University neurobiologist sparked Chile’s Senate to draft a bill to regulate how neurotechnology could be used and how data would be safeguarded.
“Scientific and technological development will be at the service of people,” the amendment promised, “and will be carried out with respect for life and physical and mental integrity.”
Chile’s new Constitution was voted down in September, effectively killing the neuro-rights bill. But other countries are considering similar legislation. In 2021, France amended its bioethics law to prohibit discrimination due to brain data, while also building in the right to ban devices that modify brain activity.
Fins isn’t convinced this type of legislation is wholly good. He points to people like Greg – the 38-year-old who regained his ability to communicate through a brain implant. If it’s illegal to alter or investigate the brain’s state, “then you couldn’t find out if there was covert consciousness”– mental awareness that isn’t outwardly apparent – “thereby destining people to profound isolation,” he says.
Access to neurotechnology needs protecting too, especially for those who need it to communicate.
“It’s one thing to do something over somebody’s objection. That’s a violation of consent – a violation of personhood,” says Fins. “It’s quite another thing to intervene to promote agency.”
In cases of minimal consciousness, a medical surrogate, such as a family member, can often be called upon to provide consent. Overly restrictive laws could prevent the implantation of neural devices in these people.
“It’s a very complicated area,” says Fins.
The Future of Brain Implants
Currently, brain implants are strictly therapeutic. But, in some corners, “enhancement is an aspiration,” says Dubljevic. Animal studies suggest the potential is there. In a 2013 study, researchers monitored the brains of rats as they navigated a maze; electrical stimulation then transferred that neural data to rats at another lab. This second group of rodents navigated the maze as if they’d seen it before, suggesting that the transfer of memories may eventually become a reality. Possibilities like this raise the specter of social inequity, since only the wealthiest may afford cognitive enhancement.
They could also lead to ethically questionable military programs.
“We have heard staff at DARPA and the U.S. Intelligence Advanced Research Projects Activity discuss plans to provide soldiers and analysts with enhanced mental abilities (‘super-intelligent agents’),” a group of researchers wrote in a 2017 paper in Nature. Brain implants could even become a requirement for soldiers, who may be obligated to take part in trials; some researchers advise stringent international regulations for military use of the technology, like the Geneva Protocol for chemical and biological weapons.
The temptation to explore every application of neurotechnology will likely prove irresistible for entrepreneurs and scientists alike. That makes precautions essential.
“While it’s not surprising to see many potential ethical issues and questions arising from use of a novel technology,” a team of researchers, including Dubljevic, wrote in a 2020 paper in Philosophies, “what is surprising is the lack of suggestions to resolve them.”
It’s critical that the industry proceed with the right mindset, he says, emphasizing collaboration and making ethics a priority at every stage.
“How do we avoid problems that may arise and find solutions prior to those problems even arising?” Dubljevic asks. “Some proactive thinking goes a long way.”
Abnormal blood clotting was one of the first mysterious health effects to emerge in the COVID pandemic, first, as an effect of the natural infection, and later, as a side effect of the COVID jabs.
By mid-March 2021, barely four months after the rollout of the COVID injections, 19 European countries plus Thailand1 had suspended the use of AstraZeneca’s injection, either in full or in part, following reports of deadly blood clots.2,3
Contrary to the Moderna and Pfizer shots, the AstraZeneca jab uses a viral vector — a genetically modified and supposedly noninfectious chimpanzee cold virus — to deliver double-stranded DNA for the SARS-CoV-2 spike protein into your cells.4
Earlier that month, The Defender had reported5 U.K. data showing the AstraZeneca jab was responsible for 77% more adverse events and 25% more deaths than the Pfizer shot. Around that same time, doctors at Oslo University Hospital also announced that the blood clotting disorders experienced by some recipients of the AstraZeneca shot were in fact caused by the injection.6 A March 18, 2021, article in Science Norway read, in part:7
“‘Our theory that this is a powerful immune response most likely triggered by the vaccine, has been confirmed,’ says professor and chief physician Pål Andre Holme … ‘In collaboration with experts in the field from the University Hospital of North Norway HF, we have found specific antibodies against blood platelets that can cause these reactions … the chief physician explains …
When asked to clarify why he says ‘most likely’ in the quote, Holme confidently responds that the reason for these rare cases of blood clots has been found.
‘We have the reason. Nothing but the vaccine can explain why these individuals had this immune response,’ he states. [Norwegian national newspaper] VG also asks how Holme can know that the immune response is not caused by something other than the vaccine.
‘There is nothing in the patient history of these individuals that can give such a powerful immune response. I am confident that the antibodies that we have found are the cause, and I see no other explanation than it being the vaccine which triggers it,’ he responds.”
Study Details Mechanism of Action
In early December 2021, a team of international scientists published a paper8 detailing the mechanism behind the AstraZeneca jab’s propensity to trigger blood clots. As reported by the Daily Mail at the time:9
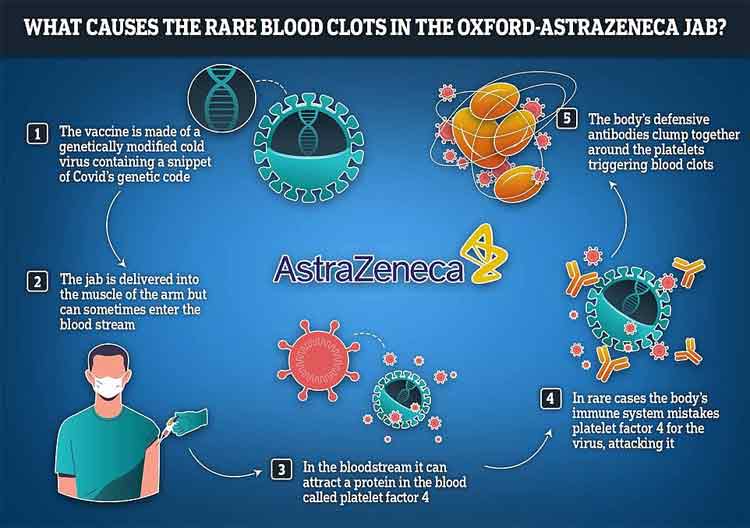
“A team of international experts, involving researchers from AstraZeneca, say that in a very small number of cases — about one in 100,000 in the UK — the vaccine can set off a chain reaction which leads to the body confusing its own blood platelets for fragments of virus …
They found that the shell of the vector vaccine — the weakened cold virus used to teach cells how to neutralize COVID — sometimes acts like a magnet and attracts platelets, a protein found in the blood.
For reasons the scientists are still probing, the body then mistakes these platelets as a threat and produces antibodies to fight them. The combination of the platelets and the antibodies clumping together leads to the formation of dangerous blood clots …
Essentially, after being delivered into the body adenovirus binds with a specific protein in the blood, known as platelet factor 4 (PF4), which is normally used by the body to promote coagulation in case of injury.
Using incredibly detailed images of the adenovirus in the vaccine the scientists demonstrated the adenovirus in the Oxford-AstraZeneca is negatively charged, and could attract positively charged proteins like a magnet.
The researchers believe that in a case of ‘mistaken identity’ the body’s immune system considers this platelet cluster as threat and releases antibodies to attack it, clumping together to it and triggering potentially life threatening blood clots. This condition is called vaccine-induced immune thrombotic thrombocytopenia (VITT).”
The following graphic was published in the Daily Mail to illustrate the potentially deadly chain reaction.
How Long Does Risk Remain?
As for how long the risk of blood clotting remains is unknown. In mid-September 2022, the American Heart Association reported that the risk of abnormal blood clotting remains elevated nearly a year after natural infection:10
“People who got COVID-19 had a higher risk of dangerous blood clots for close to a year later, according to a large new study11 on the aftereffects of a SARS-CoV-2 infection …
COVID-19 was linked to a sharply increased risk of blood clot-related issues — including heart attack and stroke — immediately after diagnosis compared to people who never had COVID-19 [and] … that risk remained higher for some problems up to 49 weeks later …
Researchers found that the first week after a COVID-19 diagnosis, the risk of an arterial blood clot — the kind that could cause a heart attack or ischemic stroke by blocking blood flow to the heart or brain — was nearly 22 times higher than in someone without COVID-19. That risk dropped sharply, to less than four times higher, in the second week.
‘Between 27 and 49 weeks, there is an approximately 30% increased risk for arterial clots,’ [senior author, professor of medical statistics and epidemiology at the University of Bristol, Jonathan] Sterne said. ‘But the elevation is greater for longer’ for clots in veins, which include deep vein thrombosis and pulmonary embolism, when a clot travels to the lungs.
In the first week after a COVID-19 diagnosis, the risk of such venous problems was 33 times higher. By the third and fourth weeks after diagnosis, the risk was still about eight times higher. And between 27 and 49 weeks later, the risk was still 1.8 times higher than in somebody who had never had COVID-19.”
If the risk of blood clotting remains high for nearly a year after natural infection, it seems reasonable to suspect the risk is dramatically elevated far longer in those who got one or more COVID shots, as their bodies are now producing the toxic spike protein internally, and there’s no known off-switch.
We still do not know how long the human body continues to produce spike protein after a COVID jab. And, while AstraZeneca was singled out as the main culprit of blood clots, Pfizer’s and Moderna’s mRNA jabs are no safer in this regard.
Pfizer’s COVID Jab Linked to Blood Clotting Disorder
As early as June 2021, Israeli research suggested there was a link between the Pfizer shot and thrombotic thrombocytopenic purpura (TTP), which is very similar to vaccine-induced immune thrombotic thrombocytopenia or VITT. A list of distinguishing features between the syndromes can be found on UpToDate.com.12 As reported by The Defender:13
“Scientists with the Institute of Hematology at Shamir Medical Center said they began researching the possible link after reports of a sudden increase in TTP across Israel — four cases detected in one month compared to two or three cases per year. TTP is an autoimmune disorder that causes blood clots to form in small blood vessels throughout the body …
The medical team said they found a ‘chronological connection’ between vaccination and the onset of TTP symptoms. They stressed this occurred in both new patients and in patients with pre-existing TTP whose disease had been in remission but flared up soon after getting the vaccine …
As The Defender reported in April, U.S. regulatory officials were alerted as far back as December 2020 that the Pfizer and Moderna vaccines — like AstraZeneca and J&J COVID vaccine — could pose similar risks of blood clots.”
Even before the rollout of the shots, experts warned that blood clots and cardiovascular problems were predictable. Among them were Dr. Patrick Whelan, a pediatric specialist, who in a letter14 to the U.S. Food and Drug Administration warned that the shots could “cause microvascular injury and blood clots throughout the body including the brain, heart, liver and kidneys, in ways that were not assessed in the safety trials.”
He pointed out that studies looking at the natural infection had found that “viral proteins appear to cause tissue damage without actively replicating virus,” and if that was true, he suspected the spike protein produced in response to the jabs might also cause the same kind of damage. Today, ample evidence points to Whelan’s suspicions being correct.
Jabs May Raise Risk of COVID Death Over Time
Studies are now also coming out with evidence that the shots may be causing antibody dependent enhancement (ADE), and that they kill heart and brain cells. Starting with the ADE evidence, a Swedish study,15 using data from the entire Swedish population over the age of 12, a total of 9,153,456 people, found that two doses were 43% protective against Omicron infection at week 4. By week 14, protection had dropped to zero.
Effectiveness against COVID-related hospitalization remained around 80% until week 25, but dropped to 40% by week 40. While these data are highlighted in the abstract, a more intriguing finding remains buried in the text that few take the time to read. As reported by investigative journalist Alex Berenson:16
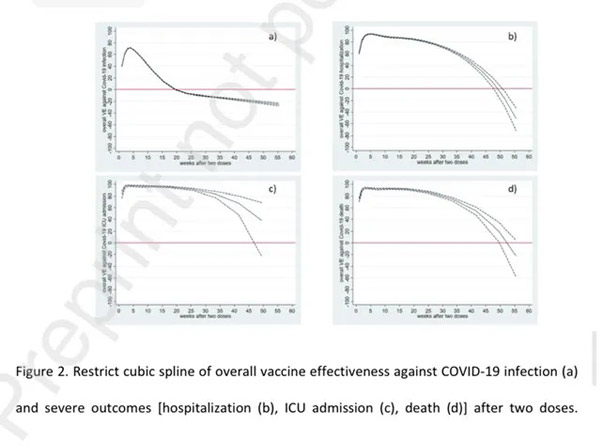
“Based on one statistical analysis [cubic spline method] vaccinated people had a HIGHER risk of death or hospitalization from COVID roughly a year after receiving their second dose. The charts — b and d below — show that vaccine protection against death and hospitalization begins to decline slowly after about five months and then plunges about nine months …
This data provides real-world evidence of possible vaccine-caused ‘antibody dependent enhancement.’ In ADE, vaccines cause our immune systems to produce antibodies that help a virus or other pathogen to attack us …
(The top chart shows the relative risk of infection, hospitalization, intensive care, and death by week after two vaccine doses. The red line marks zero effectiveness; when the blue line falls below it, it is suggesting vaccinated people are at higher risk of infection.)”
When they used another statistical method called standard polynomial regression, the shots remained moderately effective against hospitalization and death over time, falling to 45% protection against death around nine months, after which the effectiveness mysteriously started trending upward again.
According to Berenson, the lead author of the paper did not endorse either method as superior to the other. When asked for comment, Dr. Yiyi Xu told Berenson they “need more data to know which finding might be correct,” and that, at present, “the estimation is quite uncertain for both analyses.”
COVID Shots Kill Brain and Heart Cells
Another recent paper17 links the COVID shots to lethal myocarditis (heart inflammation) and encephalitis (brain inflammation). As reported by Steve Kirsch:18
“The paper is entitled: ‘A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19.’ It was published yesterday, Oct 1, and … already has over 100,000 views of the abstract and over 6,000 views of the full text.”
The report details the case of a 76-year-old man with Parkinson’s disease (PD) who died three weeks after receiving his third COVID shot. His first injection was the AstraZeneca jab, received in May 2021, which was followed by two doses of Pfizer in July and December 2021 respectively.
Autopsy confirmed his Parkinson’s diagnosis, but it also revealed several unexpected conditions contributing to his death, including:
Aspiration pneumonia
Systemic arteriosclerosis
Acute vasculitis (vascular inflammation) in both the brain and the heart
Multifocal necrotizing encephalitis (meaning tissue death all over the brain)
Chronic cardiomyopathy (heart disease), and
Mild acute lympho-histiocytic myocarditis (a rare form of myocarditis that occurs wen lymphocytes, white blood cells, enter and inflame the heart muscle)
Testing for SARS-CoV-2 antigens (spike and nucleocapsid proteins) revealed the inflammation was in response to spike protein only, particularly in the endothelial cells of small blood vessels. As noted by the authors:19
“Since no nucleocapsid protein could be detected, the presence of spike protein must be ascribed to vaccination rather than to viral infection. The findings corroborate previous reports of encephalitis and myocarditis caused by gene-based COVID-19 vaccines.”
Kirsch goes on to cite other evidence showing the COVID shots can kill, including a report20 titled “On COVID Vaccines: Why They Cannot Work, and Irrefutable Evidence of Their Causative Role in the Deaths After Vaccination,” written by Drs. Sucharit Bhakdi and Arne Burkhardt.
Bhakdi and Burkhardt claim to have developed a way to test for spike protein in human tissue, and say they’ve found spike protein in the tissues of people who have been injured and/or killed by the jabs.
Of the 15 bodies their team examined for this report — all of whom had died seven days to six months post-jab — 14 (93%) were found to have been killed by the COVID shot.21 The video above reviews their findings. All 14 had clear evidence of the body attacking itself, including the heart, with fatal consequences.
Resources for Those Injured by the COVID Jabs
If you got one or more jabs and suffered an injury, first and foremost, never ever take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your system. The same goes for anyone who has taken one or more COVID jabs and has had the good fortune of not experiencing debilitating side effects.
Your health may still be impacted long-term, so don’t take any more shots. When it comes to treatment, there are still more questions than answers, but many of the treatments that worked against severe COVID-19 infection also seem to ameliorate adverse effects from the jab. This makes sense, as the toxic, most damaging part of the virus is the spike protein, and that’s what your whole body is producing if you got the jab.
Both agree that eliminating the spike protein your body is now continuously producing is a primary task. Perro’s preferred remedy for this is hydroxychloroquine, while Kory typically uses ivermectin. Both of these drugs bind and thereby facilitate the removal of spike protein.
As a founding member of the Front Line COVID-19 Critical Care Alliance (FLCCC), Kory helped develop the FLCCC’s post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com22 (hyperlink to the correct page provided above).
Other Helpful Treatments and Remedies
In previous articles, I’ve also covered a number of treatments and remedies that can be helpful for COVID jab injuries, such as:
• Time-restricted eating — Kory believes there may be ways to boost the immune system to allow it to degrade and eventually remove the spike from your cells naturally, over time. One of the strategies he recommends for this is TRE (time restricted eating), which stimulates autophagy, a natural cleaning process that eliminates damaged, misfolded and toxic proteins. Another strategy that can do the same thing would be sauna therapy.
Most people eat more than 12 hours a day, which is a recipe for metabolic disaster. The ideal window for most everyone is 16 to 18 hours of continuous fasting with the least meal at least three hours before bed. If you are overweight, shoot for 18 hours of fasting each day; if you’re of normal weight, 16 hours.
• Lower your omega-6 intake — Linoleic acid is consumed in amounts 10 times above the ideal in well over 95% of the population, and contributes to massive oxidative stress that impairs your immune response. Seed oils and processed foods need to be diligently avoided. You can review this previous post for more information.
• Pharmaceutical grade methylene blue, which improves mitochondrial respiration and aid in mitochondrial repair. At 15 to 80 milligrams a day for those suffering from long-haul COVID could go a long way toward resolving some of the fatigue many suffer post-jab. Methylene blue is actually the parent molecule for hydroxychloroquine and has been used to treat malaria since 1890.
It may also be helpful in acute strokes. The primary contraindication is if you have a G6PD deficiency (a hereditary genetic condition), in which case you should not use methylene blue at all. To learn more, see “The Surprising Health Benefits of Methylene Blue.”
• Near-infrared light, as it triggers production of melatonin in your mitochondria23 where you need it most. By mopping up reactive oxygen species, it too helps improve mitochondrial function and repair. Natural sunlight is 54.3% infrared radiation,24 so this treatment is available for free. For more information, see “What You Need to Know About Melatonin.”
Xarelto (rivaroxaban) is a blockbuster blood thinning medication that’s been prescribed more than 80 million times in the U.S. alone.1 But the drug, which is manufactured by the Janssen Pharmaceuticals division of Johnson & Johnson, may have been approved based on manipulated data.
The research in question was published by researchers with Temple University in Philadelphia. In August 2022, The Journal of American College of Cardiology (JACC) retracted a paper2 that concluded Xarelto “could have a healing effect on hearts.”3
In addition to the retracted research study, the Journal of Molecular and Cellular Cardiology and the Journal of Biological Chemistry are investigating five more papers by the Temple University team.4
The U.S. Office of Research Integrity (ORI), which oversees research integrity activities on behalf of the Secretary of Health and Human Services, including oversight of research misconduct inquiries and investigations,5 also requested in September 2020 that Temple University investigate the research.
As a result, Temple University is also looking into 15 papers published from 2008 to 2020, which received grant money from the U.S. National Institutes of Health.6
Is Fraudulent Data Behind Blockbuster Heart Drug Xarelto?
The JACC Journals Ethics Board voted to retract the Temple University study after a reader raised concerns about several Western blot images that were used. Western blotting is a technique used to detect the presence of a protein extracted from cells or tissue.7
The editorial board requested a response from the researchers, and they sent original images as a replacement. Initially, the journal published a correction in September 2020, but according to JACC:8
“The correction raised further concerns about the image data. After an external evaluation, the decision to retract the paper is based on concerns regarding the splicing and/or duplication of Western blot images … None of the apparent splices were indicated in the arrangement of the figures.”
The retraction, however, is only the beginning. Of the 15 Xarelto papers being investigated by Temple University, nine were supervised by Abdel Karim Sabri, a professor at the university’s Cardiovascular Research Center. Sabri’s colleagues, Steven Houser, a former president of the American Heart Association and senior associate dean of research at Temple, is an author of five of these studies, along with another four studies being investigated.
In 2021, Houser filed a lawsuit to stop Temple University’s inquiry and denied falsifying data or engaging in scientific misconduct. According to Reuters, Houser believes “Temple sought to discredit him and steal his discoveries.”9
A Temple spokesperson told Reuters that it’s still reviewing the allegations. However, the lack of standardization in misconduct reviews is glaring. Even though the research is subject to fraud investigations, Janssen Pharmaceuticals was reportedly unaware of the inquiries or the study retraction by the JACC.
Meanwhile, the journals that have published the research studies being reviewed for misconduct have not published any “expressions of concern,” which inform readers that there may be reason to doubt the results. Further, five of the studies have been published in American Heart Association (AHA) journals where Houser acts as a senior advisory editor. Reuters reported:10
“The AHA said it had not been notified by the U.S. agency or by Temple about their inquiry, and that it does not view itself as responsible for investigating further. The AHA said it had issued a correction of data on one paper at the authors’ request. The paper was the sole study under scrutiny that listed Houser as supervising researcher.”
NIH Funding Potentially Fraudulent Research
An analysis of NIH grants by Reuters revealed that Houser received close to $40 million in NIH funding while Sabri received nearly $10 million.11 A separate Reuters investigation revealed in June 2022 that NIH spent at least $588 million on research into whether heart stem cells could regenerate human hearts.
In 2013, the government became aware of misconduct in the field; a leading researcher, Dr. Piero Anversa, was accused — and later found guilty — of fabrication of data and “deliberately misleading record-keeping.”12 According to Reuters:13
“Yet federal money has continued to flow to test the proposition advanced by Anversa — that adult stem cells can regenerate or heal hearts. Over two decades, federal and private grants have streamed into research labs despite allegations of fraud and fabrication against Anversa and others in the field, Reuters found.
Meanwhile, no scientist has credibly established that Anversa’s regeneration hypothesis holds true in humans, according to researchers and a review of medical literature.
Since 2001, the U.S. National Institutes of Health spent at least $588 million on such heart research, Reuters found in an analysis of government data. More than $249 million, about 43% of the total, has been awarded since March 2013. By that time, the federal government had been informed of the fabrication allegations against Anversa, according to documents and interviews with sources familiar with the matter.”
Brigham and Women’s Hospital in Boston, where Anversa’s lab was located, agreed to pay back $10 million to NIH, which is only about one-fourth of what the lab received for Anversa’s heart stem cell research.14 It’s unknown whether Temple will be required to return federal funding for the research retracted by the JACC.
Deadly Bleeding Episodes Lead to $775 Million Settlement
Xarelto is taken to thin the blood to prevent blood clots and strokes. However, it can trigger deadly bleeding, an adverse effect that consumers weren’t adequately warned about. The episodes were serious and common enough that, in 2018, the U.S. Food and Drug Administration approved Andexxa to act as an antidote to stop bleeding caused by Xarelto.15
About 25,000 lawsuits were filed against Johnson & Johnson and Bayer, which jointly sell Xarelto, claiming that the companies failed to warn patients about the drug’s potentially fatal bleeding risks. Although they did not admit liability, the companies agreed to pay $775 million to settle the lawsuits in 2019.
Further, in 2016, a blood testing device was recalled that was used in Xarelto’s ROCKET-AF clinical trial, which provided “the primary data to support the 2011 approval” of the drug. The device, which was later found to be faulty and capable of generating inaccurate results, was used in the Xarelto trial to monitor warfarin therapy in the control group.16
Although the FDA concluded that the trial results were not affected by the faulty monitoring device, the lawyers for the plaintiffs in the Xarelto lawsuits questioned whether the study’s results were skewed.17
Xarelto Linked to Greater Bleeding Risks
If you’re taking Xarelto, you should know that a nationwide population-based cohort study published in 2021 found that, compared to other direct oral anticoagulants (DOACs), Xarelto was associated with higher rates of gastrointestinal bleeding.18
Specifically, compared to Eliquis (apixaban), manufactured by Bristol-Myers Squibb, Xarelto was 46% more likely to cause gastrointestinal bleeding. According to lead study author Dr. Arnar B. Ingason with the University of Iceland, Reykjavik:19
“We had this theory that rivaroxaban would have potentially higher risks of GI bleeding because it’s given as a once-daily dose, compared to the other two drugs, which are given twice daily. Theoretically, this should cause greater variance in drug plasma concentration, making these patients more susceptible to bleeding.”
A 2016 study found similar results, noting, “In a population-based study of patients receiving DOAC agents, we found apixaban had the most favorable GI safety profile and rivaroxaban [Xarelto] the least favorable profile.”20
Dr. Neena S. Abraham, who led the 2016 study, told TCTMD, “I don’t think further investigation is needed on this topic. The data from the last four years overwhelmingly show that rivaroxaban is most likely to cause gastrointestinal bleeding. This finding is consistent among all age groups.”21
Natural Strategies for Blood Clot Prevention
Blood clotting has been described as the basic underlying pathological process that causes all heart disease. In almost everyone, the process of endothelial damage and blood clotting is an ongoing process, which means that problems only occur when the damage/blood clotting process occurs faster than the repair process, at which point you will end up with plaque buildup.
This thickens the arterial wall, forcing blood flow through a narrower gap. When a large blood clot forms on top of an existing plaque in this already narrowed area, you can end up with a heart attack or stroke.
In my interview with Dr. Malcolm Kendrick, a board-certified family physician and author of the book, “The Clot Thickens: The Enduring Mystery of Heart Disease,” he details solid strategies for lowering your thrombotic risk. Here’s a short-list of examples covered in far greater depth in the book, as well as some of my own recommendations that I bring up in the interview:
Avoid unnecessary use of nonsteroidal anti-inflammatories (NSAIDs) such as ibuprofen, aspirin and naproxen — While they effectively inhibit inflammation, they can cause platelet aggregation by blocking COX-2. In other words, they activate your blood clotting system, making blood clots more likely.
Get plenty of sensible sun exposure — Sun exposure triggers NO that helps dilate your blood vessels, lowering your blood pressure. NO also protects your endothelium, and increases mitochondrial melatonin to improve cellular energy production.
Avoid seed oils and processed foods — Seed oils are a primary source of the omega-6 fat called linoleic acid (LA), which I believe may be far more harmful than sugar. Excessive intake is associated with most all chronic diseases, including high blood pressure, obesity, insulin resistance and diabetes.
LA gets embedded in your cell membranes, causing oxidative stress, and can remain there for up to seven years. Oxidative linoleic acid metabolites (OXLAMs) are what’s causing the primary damage, including endothelial damage.
Lower your insulin and blood sugar levels — Simple strategies to accomplish this include time-restricted eating, eating a diet high in healthy fats and low in refined carbohydrates, significantly restricting your LA intake and getting regular exercise.
Address chronic stress, which raises both blood sugar and blood pressure, promotes blood clotting and impairs your repair systems. Cortisol, a key stress hormone, reduces endothelial cell production.
Quit smoking.
Natural Alternatives to Blood Thinners
Xarelto, in particular, is often prescribed for people with certain types of atrial fibrillation (AFib). AFib is an abnormal, often rapid, heart rhythm that occurs when the atria, your heart’s upper chambers, beat out of sync with the ventricles, the heart’s lower chambers. It’s a common symptom in those with heart failure or heart disease but can also occur on its own.
Oxidative stress and increased ROS can play a role in the development of AFib. Conversely, scavenging of ROS and a reduction in oxidative stress have been shown to be an essential part of keeping the heart functioning normally.22 Toward this end, CoQ10 has been found to help improve AFib.23 For older adults, ubiquinol, the reduced version of CoQ10, is more readily absorbed.
Another option for those looking to avoid Xarelto’s risks — as we await the findings of the broadening inquiries into potential research misconduct — is lumbrokinase, a complex fibrinolytic enzyme extracted from earthworms. As noted in the Institute for Progressive Medicine, this represents a potentially safer option for thinning your blood naturally:24
“Generally, we are better off with blood that clots less easily … Individuals at high risk of forming clots, such as those with atrial fibrillation, are often treated with blood thinners like aspirin or stronger agents like Coumadin … All of these agents, however, present a significant risk of bleeding, and may themselves cause brain hemorrhage, urinary or gastrointestinal bleeding.
Lumbrokinase … reduces coagulation by lowering blood viscosity, lowering the activity of clotting factors including fibrinogen, and degrading fibrin, a critical factor in clot formation. It has a stronger effect on reducing blood viscosity than other enzyme preparations.”
Winter is coming. Do you know what that means? Cuffing season is upon us. And if you happen to follow #cuffingseason, you’ll learn that September is “Drafting” and October is the “Tryout” phase.
It has nothing to do with sports. It’s all about dating during this time of year.
“Cuffing season is the search for someone to shack up with or exclusively date during the holidays and colder winter months,” says Samantha Burns, a psychotherapist and dating coach and author of Done with Dating: 7 Steps to Finding Your Person. “It’s a time when casual dating shifts to more exclusive, committed dating. It’s about enjoying the warmth of a cuddle buddy instead of venturing out into the cold to meet up with potential dating duds,” she says.
There isn’t hard scientific data on the dating trend, some outlets have attempted to quantify it. In one survey by the dating app Coffee Meets Bagel, about half of singles surveyed said they think more about dating during cuffing season, and 4 in 10 say they’re more likely to use dating apps during this time. One-fifth of survey respondents said they’d date someone in the winter to avoid being lonely, according to data analytics firm YouGov. (This survey focused on cuffing being a conscious short-term fling, but of course these relationships can last longer.)
While the term might sound lighthearted and fun, the drive to get cuffed is based on a deep, natural human need, says psychologist Lisa Marie Bobby, PhD, host of the Love, Happiness & Success podcast. “In the summer, people are flittering around like dragonflies. In the winter, at least in the Northern hemisphere, it’s cold and dark, and it can feel very lonely,” she says. “There’s this evolutionary pull to connect with other humans, which is often subconscious.”
Not to mention, no matter where you live, the holidays – with all their family events and parties – are looming. Simply seeing the decorations out in stores can prime you to seek connection, Bobby says. That’s especially true if you want to be able to shut down your always-critical aunt at the Thanksgiving table. (Yes! I have found someone!) And if one of your goals this year was to find a partner, now you’re on a deadline – and that might make you even more enthusiastic to get out there.
No matter what your motivation, it’s valid and useful. “Finding the right person requires a lot of energy and effort,” Bobby says. Cuffing season can give you that extra push you need.
How Long Can Cuffing Last?
Cuffing, while it may be seasonally motivated, isn’t always a temporary fling. For some, that’s the case: You want a person to be your plus one for the holidays. “The relationship could fizzle out come spring, but you could also genuinely fall in love and create a long-lasting relationship,” Burns says.
There’s also an opportunity to get to know people on a deeper level during this time of year. “It always takes a long time to really get to know someone,” Bobby says. “To connect and develop a relationship during a quieter time of year is to your advantage, since it can help you get to know someone on a more meaningful level.”
Ordering in just the two of you or cuddling on the couch, for instance, may set the stage for deeper conversations. At the very least, being one-on-one helps you determine if you really enjoy spending time with this person and if their goals and values are in line with yours. And if you bring them around the family for the holidays (or you go to theirs)? That’s another way to deepen that connection and get a sense on if this is a true fit or not. By the time spring comes around, you’ve had enough time to know if you’d like to continue.
Cuff Considerately
Whether winter is coming or it’s smack dab in the middle of summer, it’s important to keep a few things in mind for a healthy partnership.
Communicate: Don’t know your new partner’s intentions with the relationship? Burns urges you to open up the lines of communication to get on the same page. You may want a long-term commitment, but what if they want something casual? Hopefully, they’re open to answering questions about where you two stand, but if they dodge or shut down the convo, that’s your indication that they’re not taking things as seriously as you are, she says. It will be up to you to decide if you’re OK with that. Similarly, if you’re at relationship crossroads and don’t want to be with the person you’re cuffed with any longer, then it’s important to be clear and break up (no ghosting).
Open up: It’s not just The Bachelor franchise that has a trademark on getting vulnerable. In fact, if you are trying to find Your Person during cuffing season, Burns suggests having meaningful, vulnerable conversations during the first few dates. That includes big questions, such as having kids (and raising them!), what your political beliefs are, what you want out of life, and much more. This has a dual purpose: “This is how you can not only create deeper emotional intimacy and form connection,” Burns says, “but also make sure you’re not wasting your time with someone who will only be around for one season, or who doesn’t want the same things.”
Work on yourself: Before cuffing season kicks off, it’s a great time to do the inner work that can help foster attracting the right partner and building healthy relationships, Bobby says. “Getting clear about who you are and your values and gaining self-awareness about your patterns in relationships is personal growth work that can help you make good decisions.”
I’ve seen hiccups in the process of diagnosing psoriatic disease. I also know about it firsthand. I’m 62 years old, and I’ve had psoriasis since I was a teenager.
I first got it when I was 15. Not too long after that, when I was 17, I started to have pain in my lower back. I had years of appointments, doctor visits, and tests, but I didn’t discover that psoriatic disease had affected my joints until I was 30.
Once, when my psoriasis flared, I decided to see a dermatologist. They recognized I had joint inflammation and then referred me to a rheumatologist. It was then that I found out I had psoriatic disease involving my joints. So it took more than 10 years to get a proper diagnosis once I started to have symptoms.
My doctor didn’t connect my skin problems with the joint trouble I was having.
If you have psoriatic disease, the sooner you can get an accurate diagnosis, the better. In my case, the slow diagnosis meant I didn’t get the right treatment right away. That left me with joint changes and fused bones, mainly in my feet, back, and neck. Early diagnosis might have helped me avoid the disability that stemmed from that.
With psoriatic disease, it’s common for symptoms to be missed and diagnoses to take a long time. Symptoms often go unreported or overlooked for a variety of reasons.
I’ve learned that often comes from a lack of awareness about the link between the skin and joint involvement. You may think of skin lesions as an external disease and joint inflammation as an internal one. But actually, they’re both autoimmune disorders related to your immune system.
Why Psoriatic Disease Symptoms Get Missed
It’s common to misunderstand skin issues. You may think you have dandruff when it’s really scalp psoriasis. It’s also common not to report problems with your nails, which may be nail psoriasis. Your medical chart may reflect dry skin or eczema. If you see a new doctor, they might not think to ask about signs or symptoms of psoriatic disease.
You also may not think symptoms like joint pain, swelling, and fatigue have anything to do with your skin issues. That’s especially common with younger people, who are less likely to think that joint pain is something that can happen to them.
It’s best to let your doctor know about all symptoms you have.
Other Reasons Symptoms Get Missed
Symptoms of psoriatic disease also go unreported because they can often be vague. Test results or X-rays may not show anything. What you feel may not seem to change much over time. You might dismiss or doubt your symptoms because they’re not obvious or consistent.
Symptoms might also be intermittent — they may come and go. If you go to the doctor when things like joint pain or swelling aren’t happening, you may not think to tell your doctor about them.
What You Can Do
Report all symptoms to your doctor, regardless of whether you think they’re connected to your psoriasis. Make sure you consider symptoms you’ve had before, even if you don’t have them when you go to your appointment.
Think about your family history. Do any family members have conditions that might have gone misdiagnosed? Do they have symptoms that could relate to psoriatic disease?
Remember that psoriasis skin symptoms are a visual sign that something may be wrong with your immune system. So it’s possible you may have other issues, like joint pain and fatigue. If you’ve had these, talk to your doctor about the possibility of psoriatic disease.