
Quercetin’s Effect on Blood Pressure



[ad_1]
Fall and winter have always been peak seasons for respiratory viruses. As the weather cools in many parts of the U.S., people are forced into indoor environments where viruses can spread more easily. Holiday gatherings and travel can also become breeding grounds for disease.
That’s one reason why experts are worried that COVID-19 case counts may rise in the U.S. in the coming weeks. But there’s also another. To help forecast COVID-19 rates for the U.S., experts often look to Europe—and the data there aren’t promising. More than 1.5 million COVID-19 diagnoses were reported across Europe during the week ending Oct. 2, about 8% more than the prior week, according to the World Health Organization’s (WHO) latest global situation report, published Oct. 5. More than 400,000 of those diagnoses came from Germany, and almost 265,000 came from France.
“We’re concerned,” said Maria Van Kerkhove, the WHO’s technical lead on COVID-19, at an Oct. 5 press briefing. “In the Northern Hemisphere, we’re entering autumn and the winter months, so we will see co-circulation of other viruses like influenza….We need health systems to be prepared.”
The U.S. doesn’t always follow in Europe’s footsteps. The Alpha variant, for example, caused a larger spike in Europe than in the U.S. But European outbreaks related to Delta and Omicron predated similar surges in the U.S.
COVID-19 in the U.S. has been at a “high-plains plateau” for months, says Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota. Since the spring, roughly 300 to 500 people have died from COVID-19 each day—a rate that is still tragically high but relatively stable.
Read More: What Happens If I Get COVID-19 and the Flu at the Same Time?
The situation in Europe “may be a harbinger of things to come,” Osterholm says. He fears a “perfect storm” may be brewing, threatening to turn that U.S. plateau into another surge. Waning immunity, low booster uptake, ever-evolving subvariants that are increasingly good at evading the immune system, and people behaving as if the pandemic is over all suggest “we are headed to the end of the high-plains plateau,” Osterholm says. “I just don’t know what [the next phase] looks like.”
Federal case counts aren’t showing an uptick in the U.S. yet; in fact, daily diagnoses and hospitalization rates have fallen steadily since July. But case counts have become increasingly unreliable as more people rely on at-home tests and states pull back on reporting. Osterholm says he pays closer attention to death and hospitalization rates, but both lag behind actual spread of the virus, since it can take time for infections to become serious enough to result in hospitalization or death.
Meanwhile, the CDC’s wastewater surveillance dashboard, which tracks the level of virus detected in wastewater samples across the country, suggests circulation is increasing in multiple parts of the country, including portions of the Northeast and Midwest.
Taken together, the signs suggest a surge is coming, says Arrianna Marie Planey, an assistant professor of health policy and management at the University of North Carolina’s Gillings School of Global Public Health.
“I don’t like to use the word ‘inevitable’ because all of this is preventable,” Planey says. “It’s just that prevention is harder and harder at this stage of the pandemic,” when mitigation measures like mask mandates have fallen away and many people either don’t know about or don’t want to get the new Omicron-specific boosters.
Planey has been encouraging people she knows to get boosted and making sure they know about tools like Evusheld (a vaccine alternative for people who are immunocompromised or unable to get their shots) and the antiviral drug Paxlovid. She says she’d like to see more urgency from the government, including stronger communication about the need to get boosted and a continued push for those who haven’t been vaccinated at all to get their primary shots.
The problem, Osterholm says, is getting people to actually heed those warnings. Many polls show that Americans are ready to leave the pandemic behind, even if the virus continues to spread and mutate in the future.
That leaves public-health experts with the frustrating job of repeating the same advice they’ve given for the last several years, to an increasingly detached audience. “There’s no joy in saying, ‘I told you so,’” Planey says, “because people are sick and dying.”
More Must-Read Stories From TIME
[ad_2]
Source link


[ad_1]
The U.S. on Wednesday authorized updated COVID-19 boosters for children as young as 5, seeking to expand protection ahead of an expected winter wave.
Tweaked boosters rolled out for Americans 12 and older last month, doses modified to target today’s most common and contagious Omicron relative. While there wasn’t a big rush, federal health officials are urging that people seek the extra protection ahead of holiday gatherings.
Now the Food and Drug Administration has given a green light for elementary school-age kids to get the updated booster doses, too—one made by Pfizer for 5- to 11-year-olds, and a version from rival Moderna for those as young as 6.
There’s one more step before parents can bring their kids in for the new shot: The Centers for Disease Control and Prevention, which recommends how vaccines are used, must sign off.
Americans may be tired of repeated calls to get boosted against COVID-19, but experts say the updated shots have an advantage: They contain half the recipe that targeted the original coronavirus strain and half protection against the dominant BA.4 and BA.5 Omicron versions.
Read More: What Happens If I Get COVID-19 and the Flu at the Same Time?
These combination or “bivalent” boosters are designed to broaden immune defenses so that people are better protected against serious illness whether they encounter an Omicron relative in the coming months—or a different mutant that’s more like the original virus.
“We want to have the best of both worlds,” Pfizer’s Dr. Bill Gruber, a pediatrician, told The Associated Press. He hopes the updated shots will “re-energize interest in protecting children for the winter.”
The updated boosters are “extremely important” for keeping kids healthy and in school, said Dr. Jason Newland, a pediatric infectious disease specialist at Washington University in St. Louis.
Parents should know “there is no concern from the safety perspective with the bivalent vaccines, whether Moderna or Pfizer,” Newland added.
Only people who’ve gotten their initial vaccinations—with any of the original-formula versions—qualify for an updated booster. That means about three-fourths of Americans 12 and older are eligible. As of last weekend, only at least 13 million had gotten an updated booster, White House COVID-19 coordinator Dr. Ashish Jha estimated Tuesday.
To pediatricians’ chagrin, getting children their first vaccinations has been tougher. Less than a third of 5- to 11-year-olds have had their two primary doses and thus would qualify for the new booster.
This age group will get kid-size doses of the updated booster—and they can receive it at least two months after their last dose, whether that was a primary vaccination or an earlier booster, the FDA said.
Pfizer said it could ship up to 6 million kid-sized doses within a week of authorization, in addition to ongoing adult-dose shipments.
Until now, Moderna’s updated booster was cleared only for adults. Wednesday’s FDA action authorized the booster for teens as well as children as young as age 6.
As for even younger tots, first vaccinations didn’t open for the under-5 age group until mid-June—and it will be several more months before regulators decide if they’ll also need a booster using the updated recipe.
Exactly how much protection does an updated COVID-19 booster shot offer? That’s hard to know. Pfizer and Moderna are starting studies in young children.
But the FDA cleared the COVID-19 booster tweaks without requiring human test results—just like it approves yearly changes to flu vaccines. That’s partly because both companies already had studied experimental shots tweaked to target prior COVID-19 variants, including an earlier Omicron version, and found they safely revved up virus-fighting antibodies.
“It’s clearly a better vaccine, an important upgrade from what we had before,” Jha said earlier this week.
Jha urged adults to get their updated shot in October—like they get flu vaccinations—or at least well before holiday gatherings with high-risk family and friends. People who’ve recently had COVID-19 still need the booster but can wait about three months, he added.
More Must-Read Stories From TIME
[ad_2]
Source link

[ad_1]
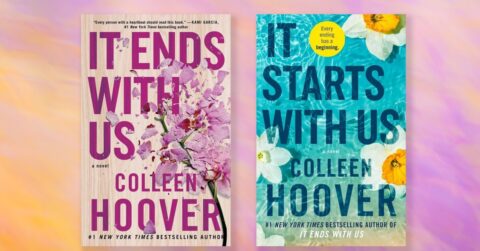
Colleen Hoover fans—a passionate group of readers who call themselves the CoHort—are preparing to be emotionally walloped.
On Oct. 18, Hoover will publish It Starts With Us, the long-awaited sequel to 2016’s It Ends With Us. While her two dozen novels are mostly romances, Hoover specializes in the type of book that practically demands a reader have their therapist on standby. Consider recent reactions on TikTok, where the #ColleenHoover hashtag has been viewed more than 2.4 billion times: “I never cry while reading books but this ending just made me burst out in tears,” one person wrote. “I’m just about to go hit rock bottom, so I was wondering if anyone needs anything while I’m there,” another chimed in, clutching a copy of It Ends With Us.
Hoover’s novels probe dark themes: abusive relationships, toxic masculinity, sexual assault, miscarriage, infidelity. She’s been open about her personal connection to some of the things she writes about: Hoover has said that her father physically abused her mother, and that It Ends With Us was inspired by her mother. The novel introduces readers to Lily—a florist who grew up with an abusive father—and her neurosurgeon husband, Ryle, who turns a childhood incident into an excuse for assaulting her. He grows especially jealous and vengeful after Lily reconnects with her first love, Atlas. When Lily learns she’s expecting Ryle’s baby, she has to decide whether she’ll continue to tolerate the cycle of abuse she’s been trapped in her entire life. It Starts With Us picks up where the novel’s epilogue ends and centers on the relationship between Lily and Atlas. It promises to deliver more of Hoover’s signature heartache and ugly tears.
Some readers have noted online that books like It Ends With Us have shifted their perspective on domestic violence, helping them understand why a battered partner might struggle to leave an abuser they still love. Hoover recalls even more personal stories from fans. “I’ve heard from readers who left terrible situations that my books inspired them to do so—that’s the most amazing thing I could ever hope to happen,” she told TIME via email. “That just sharing stories could really help change another person’s life—the weight of that is immense, but if I’ve helped one person in any way, that’s something really special.”
Hoover isn’t the only creator to be inspired by the so-called trauma plot: other examples include Hanya Yanagihara’s A Little Life, the new Netflix movie Luckiest Girl Alive, and the HBO drama Barry. Some critics pan the approach, arguing that characters are flattened when defined only by their trauma, and that it could be exploitative.
That criticism is valid, says Naomi Torres-Mackie, a psychologist at Lenox Hill Hospital in New York City and head of research at the Mental Health Coalition. “When trauma is absolutely central to a character’s existence, it can be dehumanizing and parallel what happens in real life—when we learn about somebody’s traumatic past, and they have to fear that that’s all we’ll see now,” she says. “That’s very unfortunate because, of course, trauma survivors are full, multifaceted humans.”
However, Torres-Mackie adds, when executed well, trauma has an important place in literature and media. It’s key that such depictions exist “in a way that’s holistic and humanizing and balanced.” Darkness is an inevitable part of life, she stresses: “Reading content like this can feel like a relief within a culture where we’re all supposed to be happy-go-lucky.”
Hoover self-published her first novel, Slammed, in 2012, and has since reliably churned out a couple new books a year. Much of her work has experienced a boom in popularity thanks to BookTok, the corner of the video-sharing platform TikTok dedicated to book recommendations. She authored the No. 1 and No. 2 books on the Oct. 9 New York Times best sellers list: Verity (43 weeks on the list) and It Ends With Us (68 weeks), both of which were published more than three years ago. In the past year alone, copies of her books have outsold the Bible.
It might seem counterintuitive that readers would be so eager to inhale uncomfortable books that leave them sobbing and heartbroken. But reading about trauma is appealing for a variety of reasons, one of which is that it helps us learn about the full spectrum of events that make up a life. “It gives you a lens into different experiences,” Torres-Mackie says. “As human beings, we’re inherently fascinated with each other.” In this case, that eagerness could stem from a desire to relate to people we know who have experienced trauma, or from good old-fashioned voyeurism.
There’s so much violence against women in the U.S. that it’s natural for readers to seek it out in fiction, some experts say. Forty-one percent of women have experienced sexual violence, physical violence, and/or stalking by a partner, according to the U.S. Centers for Disease Control and Prevention. “The themes in her books, while obviously dramatized and created for our entertainment, draw on a lot of what’s actually happening in this world,” says Willow Goldfarb, a Fort Lauderdale, Fla.,-based licensed mental health counselor with Thriveworks, a counseling practice with locations across the U.S. In It Ends With Us, she points out, there’s intense drama and jealousy between Lily and Ryle. Their relationship is also complex: even though Ryle’s violence is objectively unacceptable, he has a tormented but loving side that makes Lily, and some readers, wish they could rehabilitate him. “I think a lot of women can connect to that—of trying to save these men who we believe can be brought back from this brink of their own abuse and torture,” she says. Goldfarb has a point: in one TikTok video, a reader commented, “Am I the only one that wants to fix Ryle so bad?”
Readers who have experienced domestic abuse or other trauma often appreciate seeing themselves reflected back in a storyline, says Juli Fraga, a psychologist with a private practice in San Francisco. Such representation can help them feel less isolated and temper the feeling of being “other.” “They’re looking for themselves in the story,” Fraga says. “Hearing that somebody’s experiences were similar to yours, or even worse than yours, can help you feel less alone—even if it’s merely in a book of fiction.”
Others might consider the books a way to buffer their own safety and prevention strategies. A reader might watch for warning signs before Ryle shoves Lily down the stairs, cataloging his behavior before and after. Torres-Mackie explains the thought process: “If by reading these kinds of narratives I can understand this traumatic experience, even though it’s fiction, maybe I’ll be able to prevent my own pain,” she says. “There can be a sense of self-protection and learning from other peoples’ traumatic experiences.”
Hoover’s popularity speaks to a cultural shift that’s transpired over the past couple decades, says Alexandra Cromer, a Virginia-based licensed professional counselor with Thriveworks. “You didn’t talk about trauma 50 years ago,” she says. “You sucked it up and moved on.” Now, with each new generation, that’s changing. “There’s been a lot more awareness and compassion toward trauma stories—so there’s more space for people to learn about this stuff.”
Reading about trauma could certainly lead to mental-health effects, experts agree. But—and here come a therapist’s two favorite words—it depends. An individual reader’s past experiences, emotional wellbeing, and other personal factors will determine the impact a book has on them.
It’s important to consider the reason why someone is consuming this content, Torres-Mackie says. It could be the pursuit of catharsis—the healthy release of previously repressed emotions associated with traumatic events. “It can be really hard to feel difficult emotions,” she says. “But if you can experience them through somebody else, like a character in one of these books, it allows you to feel your own dark feelings.”
Especially for trauma survivors who still have a lot of healing to do, however, the material could trigger flashbacks, unpredictable emotions, physical symptoms like headaches, or even post-traumatic stress disorder. Reading about difficult subject matter, such as physical abuse, activates our mirror neurons—brain cells that are likely the neurological basis of empathy and that influence the way we experience another person’s emotions or actions. “These neurons can get fired up, and that’s why these things give you that jolt of adrenaline or excitement,” Torres-Mackie says. “You feel as if you’re in the narrative yourself.”
Torres-Mackie advises closely monitoring your reaction to the reading material: you should be consuming it, rather than having it consume you. If you start feeling hyper-vigilant and unsafe in the world, or if you’re having nightmares about the book, it’s probably smart to stop reading. Torres-Mackie offers a guiding question: “Does it fill you up, or does it deplete you?”
Ideally, readers will experience novels like It Ends With Us and It Starts With Us as what they are: entertainment, Goldfarb says. She considers herself a Hoover fan and doesn’t feel like she’s been harmed by the material. “But I’m also a person who has worked through my own trauma, and done my own therapy,” she says.
The publishing industry could do a better job of sharing resources for readers who might be adversely affected by sensitive content, she adds. “In every book, there could be a little leaflet or disclaimer, like, ‘This isn’t healthy or normal. This is for entertainment purposes,’” she suggests—plus contact information for a mental-health organization like the Substance Abuse and Mental Health Services Administration or National Alliance on Mental Illness.
Readers can also look up trigger warnings for books, including on websites like doesthedogdie.com—and these ought to be included on the cover or in some other prominent place, Goldfarb says. That would provide readers with a clear sense of whether they would encounter themes it would be healthiest for them to avoid. “Take care of yourself and tune into your body when you’re reading these things,” she says. “If you’re upset by it in a way that doesn’t go away with a cup of tea and a hug, talk to somebody about it. And let’s push for more trigger warnings about these major themes in books, so we can protect each other and still have a great time reading.”
More Must-Read Stories From TIME
[ad_2]
Source link


[ad_1]
Brandon Kapelow is a filmmaker and photographer from Wyoming. He is a suicide-loss survivor and a peer-support facilitator for SOLACE and the Greater Los Angeles chapter of the American Foundation for Suicide Prevention.
I was raised in the wilds of western Wyoming and spent my childhood exploring the foothills of the Rocky Mountains, camping in Idaho and Montana, and visiting family in Colorado and New Mexico. It was a beautiful but difficult place to grow up. Apart from Alaska, these are the states that continually rank highest for deaths by suicide, earning the Intermountain West the ominous designation “the Suicide Belt.”
My father made his first suicide attempt when I was 8 years old. He struggled for years with undiagnosed bipolar disorder and succumbed to his illness after four more attempts, in 2005 at age 64. After seeing friends and family members hospitalized or prescribed medication for suicidal ideation or attempts, I’ve come to realize how widespread this issue is for thousands of people living in small communities across the West, like the one where I grew up. Many of these Americans are struggling to process the complexities of grief that come with living through a generation or more of suicide loss, yearning for support and connection while surrounded by a culture that is rarely willing to offer or accept it.
I decided to travel to Catron County, a high-desert region in New Mexico along the Arizona border with the highest rate of suicide death of any county in the contiguous U.S. from 2010 to 2020, at 63.2 per 100,000 people. (The average national rate for the same time period was about 13.2.) I wanted to meet people who were living at the heart of this issue—to hear their stories and provide a window into their grief, as it mirrored my own. I’ve always found catharsis in talking about my experiences with suicide, and I hoped that this project might provide similar relief to those who chose to sit and speak with me. (Some asked that I omit their last names to help protect their families’ privacy.)

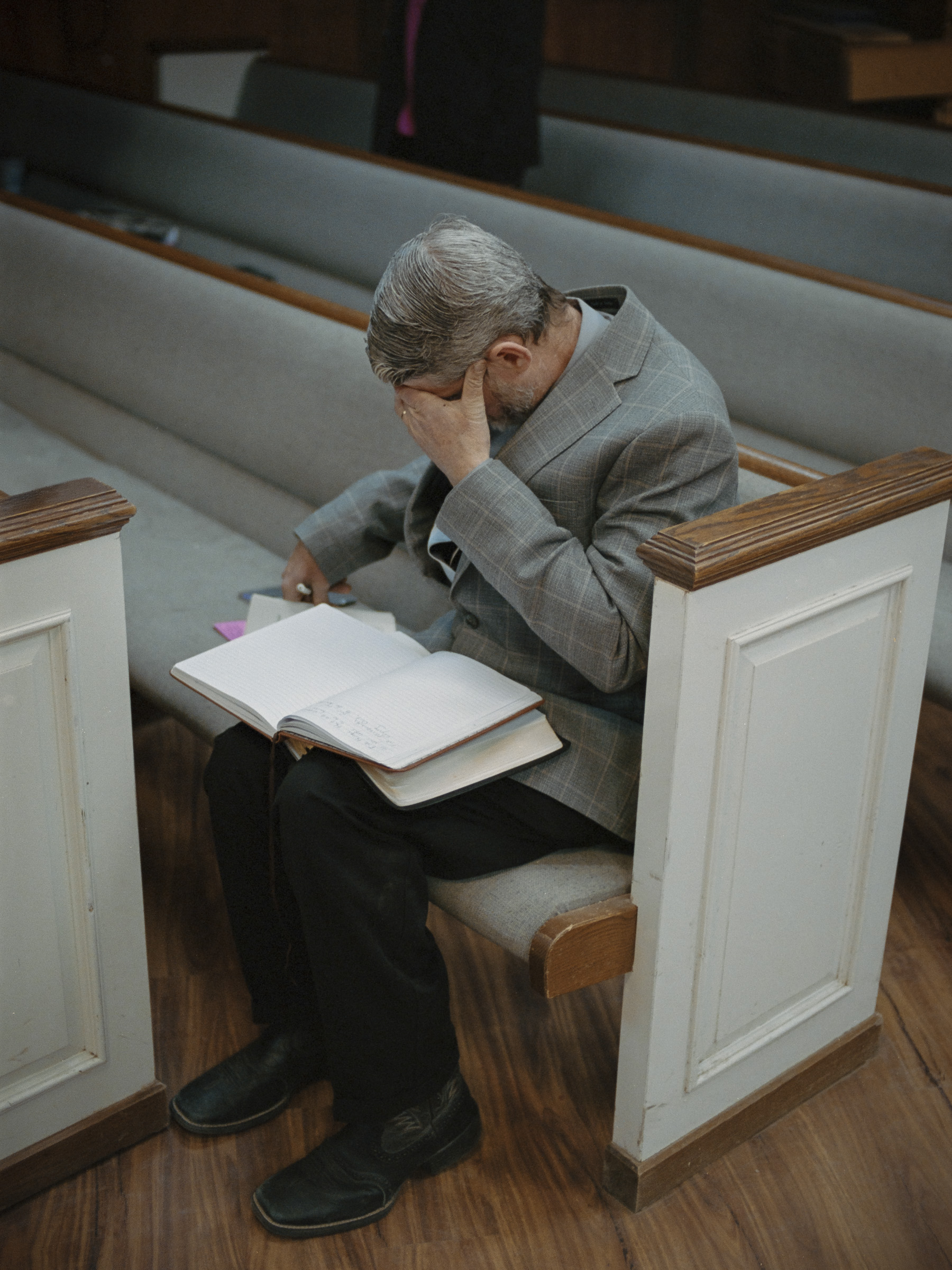
In the absence of formal behavioral-health resources, churches like the Fence Lake Community Church help people cope with suicidal ideation or grief. “A major part of my ministry—I call it group therapy on Sunday morning—is to take out of the Scriptures these verses that build people, lift people,” says Dr. Gary Knouf, a pastor at the Quemado Cowboy Church. “Almost everybody, after they leave Sunday, is full of hope.”
Brandon Kapelow

Ron, 68, is part of a four-generation ranching family and underwent several reconstructive surgeries following a suicide attempt. “It’s hard to look me in the eye, and it’s hard for folks to deal with that without a shudder going down their back,” he says. “That’s a real burden that I have from doing this. I can’t just sit down with a friend and have a drink like I used to because it makes them uncomfortable for me to be around.”
Brandon Kapelow

Cresta, 69, holds a photo of herself with her friend Dave Moller, who died by suicide in 2012. Cresta herself has also battled with periods of suicidal ideation. “Out here, we don’t have mental-health doctors. Personally, I need someone that can monitor me closely because of previous negative side effects from depression medications, such as feeling suicidal. We just don’t have those services in a rural area. The most you have is somebody who’s gone through something and helps you. That’s about it.”
Brandon Kapelow

Of the four homes on this short stretch of road in Alma, N.M., part of Catron County, two had owners who died by suicide.
Brandon Kapelow
Catron County covers a vast area of 7,000 square miles and is home to nearly 3,600 people, according to the 2020 U.S. Census. Among them are more than twice as many veterans, seniors, and Native Americans than in the average county: three groups at highest risk for suicide death. The population has experienced a 4% decline from the decade prior that reflects a national trend of urbanization that has hollowed out communities across rural America. “I spent my whole life being a cowboy, working on ranches,” Ron, the eldest of a four-generation ranching family, told me. “I think that’s why you see these rural areas having such a high incidence [of suicide]—all of a sudden, we’ve become irrelevant.” Despite a life of continuous employment in ranching, Ron struggled to make ends meet after a heart issue caused medical bills to start piling up. His financial problems and feelings of low self-worth collided, and in the winter of 2019, Ron attempted suicide.
Photographing Ron, I saw a version of my father staring back at me. He, like Ron, survived a suicide attempt that resulted in significant facial damage and spent months undergoing reconstructive surgeries and rehabilitative care before resuming a life forever altered. Meeting people like Ron often required leading with my own story, in an effort to pierce the dense clouds of stigma that still loom heavily over the West. What I didn’t expect was how often I’d find daylight.
Early in my trip I stopped at J&Y, a local auto-body shop in the town of Quemado, to get air for a leaky tire. Owner Jerry Armstrong, who also serves as the volunteer fire chief, an EMT, and a church deacon, asked what brought me to Catron; when I told him, he started to cry. One of his employees, a high school student named Thane Morgan, had taken his life just three weeks prior. Armstrong employs a number of local teens in his shop, and he worries about the ripple effects of Morgan’s suicide. “I see those kids and it’s like, How many of ’em are going to follow suit?” he told me. Morgan was not the first teen at J&Y to attempt suicide. “I feel guilty a lot of the time for even saying, ‘I’ve also been suicidal before,’ because he’s the one who actually went and did it,” says Hunter Gossett, one of Morgan’s friends at the shop. “I get the reason for wanting to do it. At the same time, I’m still here.”
Suicide contagion among teens is a real phenomenon. In the early 2010s, Reserve Independent School District in Catron County experienced a string of student suicides that prompted administrators to implement a peer-support program in which students were trained to look out for warning signs among classmates. The program was such a success that local administrators wonder if a similar program could be as effective among the county’s adult residents.
![Cathy, 69, and Dennis, 75, relax with their support dog Ricky. Cathy has lost relatives to suicide and has survived several attempts. During a recent attempt, she reached out to a hotline for help, an experience she called “a fart in a windstorm. [The responder] was quite young, and I guess I was her first active caller,” she says. “She did not know anything about elderly depression. She just knew what she had to say … 'Do you have a plan? Do you have a significant other?’ I mean, am I talking to a person? We're talking about my life.” Cathy and her husband are starting a support group called Bridge to Hope in order to bring new resources into their community. “There’s a legacy of hopelessness. And I’m trying to be a light.” (Brandon Kapelow)](https://api.time.com/wp-content/uploads/2022/09/america-suicide-highest-rates-county-cathy-dennis.jpg?quality=85&w=2400)
Cathy, 69, and Dennis, 75, relax with their support dog Ricky. Cathy has lost relatives to suicide and has survived several attempts. During a recent attempt, she reached out to a hotline for help, an experience she called “a fart in a windstorm. [The responder] was quite young, and I guess I was her first active caller,” she says. “She did not know anything about elderly depression. She just knew what she had to say … ‘Do you have a plan? Do you have a significant other?’ I mean, am I talking to a person? We’re talking about my life.” Cathy and her husband are starting a support group called Bridge to Hope in order to bring new resources into their community. “There’s a legacy of hopelessness. And I’m trying to be a light.”
Brandon Kapelow

The DWI (Driving While Intoxicated) Program in Reserve, Catron’s county seat, is one of the county’s only behavioral-health resources. Deborah Boyer, the clinic’s director and a suicide-loss survivor, sees firsthand the overlapping needs in addressing substance abuse and suicide prevention. “The stigma is horrible here. If somebody uses drugs or has attempted suicide or has mental illness, we just alienate them immediately,” she says. “We need some compassion because it ain’t working the way it’s going right now.”
Brandon Kapelow
Craig Lang, 43, is a pastor, EMT, and head organizer for the Apache Creek Deaf & Youth Ranch, a Baptist summer camp for deaf and disabled young people. In each of his roles, Lang has had extensive exposure to the traumas of suicide. A lack of emergency medical services in Catron County means that local volunteers like Craig must respond to emergencies involving neighbors or even family members.
Brandon Kapelow

Naomi Lang, 13, with her horse Duchess. Naomi’s father Craig was the closest EMT to the scene when Naomi was accidentally run over by a truck, requiring him to perform life-saving duties on his own daughter. At a national EMS conference, Craig learned that providing critical care to friends and peers can carry significant risks of developing PTSD. He had to step back from his role as an EMT after developing suicidal thoughts of his own.
Brandon Kapelow

Locals refer to a home on Main Street in Reserve as the “Death House” since two consecutive occupants died by suicide.
Brandon Kapelow
Tremendous progress in suicide prevention and mental health has been made in the U.S. in 2022. The 988 Suicide and Crisis Lifeline network was launched, and a landmark bipartisan gun safety bill passed, which strengthens red-flag laws and invests in community-based violence-prevention and behavioral-health initiatives. New federal policy changes also make telehealth services for mental-health care more accessible to people in rural areas through Medicare and Medicaid. And a recent survey published by Harris Poll found that 80% of U.S. adults report that they would tell someone if they were having thoughts of suicide—a 13% increase since 2015.
Read More: How 988 Will Transform America’s Approach to Mental Health
But it will be an uphill battle for people in Catron and similarly remote Western counties. Federal data published on Sept. 30 found that in 2021 the U.S. suicide rate rose by 4% after two years of declines. The region’s lack of resources is visible in almost every sector of public health and safety, including law enforcement, emergency medical services (EMS), and mental-health care. There isn’t a state-run hospital in the county—only a medical clinic in Reserve (the county seat) that is funded and operated by a private religious organization. The nearest Veterans Affairs (VA) clinics are several hours away. A single therapist services the region, and they don’t work with children. There’s a wellness center in Reserve, but according to staff there, locals don’t want to be seen walking in the front door.
For 911 emergencies, volunteer EMTs are often dispatched from their homes or workplaces to respond to the incident. If the issue is beyond the capabilities of the local clinic, patients are taken to hospitals in neighboring counties several hours away. The burden on first responders is particularly high due to the nature of living and working in small communities. “We know 80% to 90% of the people that we transport,” says Mike Shriver, an EMS driver and former state policeman. Mike’s wife Vicki Shriver, the Reserve district EMS medical chief, is often confronted with situations for which established protocol is insufficient. “The medical system for behavioral and psychiatric patients is broken,” she says. “There used to be a mandatory 72-hour hold for an attempted suicide … Now sometimes they’re released within 12 to 24 hours, which I don’t think gives the hospital a chance to do a complete evaluation. They’re home before I get the paperwork done.”

As a history buff, veteran, and a suicide-attempt survivor, Larry Iams, 74, maintains a careful relationship with his guns. Most of the time he keeps them locked up at a friend’s house in Arizona so that they’re out of reach.
Brandon Kapelow

After student Thane Morgan’s suicide in November 2021, administrators at Quemado High School brought in mental-health professionals to help counsel students. Years earlier, the neighboring Reserve school district had implemented a peer-support system in response to a string of teen suicides. Local officials point to the success of that program in giving students the tools and training to support one another and be alert to warning signs among peers.
Brandon Kapelow

Brenda Johnston, 49, has lost five members of her family—including her younger brother—to suicide. “There’s people that still come and ask how he’s doing,” she says. “That’s the hardest part. And they always try to ask why. I’m not going to say to suicide. To me it’s none of anybody’s business.”
Brandon Kapelow

Tristan Leyba, 16, worked with Morgan at J&Y Auto and received a farewell text from him the night that Morgan ended his life. Leyba and Morgan wore matching rings to signify their friendship.
Brandon Kapelow

Rusty Stewart, 47, a pastor at the First Baptist Church of Quemado, used to wear a gun on his hip that he described as his “backup plan.” After a suicide attempt, he was placed under observation at a hospital and told that “people who commit suicide go straight to hell,” he remembers. Stewart now uses his position at the pulpit to try to dispel stigma about mental health. “I think most depressed, suicidal people are probably closer to God than most Christians. I know because they’re the ones that are really reaching out for help.”
Brandon Kapelow
Absent a social safety net, the community must care for itself. This feeling of self-reliance is so ingrained that in 1994, Catron’s county commissioners voted unanimously to pass a nonbinding resolution that stipulated every household should have a gun. In 2019, the county commission again voted unanimously to become part of a national group of “Second Amendment Sanctuaries,” counties across the country that nullify certain gun-safety measures, such as red-flag laws, that were designed in part to help law-enforcement officers remove lethal means from people in suicidal crises.
For Larry Iams, a combat veteran and historic-gunfight reenactor, the issue of firearm safety is urgent. Iams was first attracted to Catron County because of its solitude and its support of the gun culture he cherishes. But following the death of his wife, solitude turned quickly into isolation, and a suicidal episode landed him in a VA hospital. He now locks up his guns at a friend’s home in neighboring Arizona to keep them out of reach. “People that are wanting to do this need somebody that they can trust and talk to,” he says. “That’s going to be hard sometimes because there’s not a lot of people around.”
The stark geography of Catron and other Western counties like it increases the likelihood of social isolation, another major risk factor for suicide. “There’s a lot of solitude in the West. Conditions are harsh,” says Dr. Gary Knouf, pastor at the Quemado Cowboy Church, where Morgan’s memorial service was held. “Maybe the greatest dysfunction in America is loneliness.” The experience of loneliness is not purely emotional; social isolation has harsh physical effects on the body, such as increasing stress-hormone levels, and is a risk factor for suicide.

Kathleen, 84, left, and Rose, 79, play cards at the Glenwood Senior Center. Both have lost family members to suicide. The senior center is one of the few dedicated spaces for social connection for the area’s aging population.
Brandon Kapelow

Synthetic flowers lie at the grave site of a 56-year-old man who died in January 2021 from complications related to substance abuse—but his mother believes the real cause of death was suicide. Stigma and other factors make it difficult to accurately track suicide deaths, which often leads to underreporting. According to Craig Lang, an EMT, first responders feel inclined to avoid classifying a death as a suicide in order to spare surviving family members stigma and shame.
Brandon Kapelow

Hayden Littleton, 18, was 8 years old when she lost her father James to suicide. James Littleton was 40 years old when he died in 2012. According to his daughter, James loved working with horses and running cattle, and was never seen without his signature hat, blue jeans, and a long-sleeved shirt. She is reminded of him whenever she sees images of cowboys.
Brandon Kapelow

Jack Diamond, 84, stands at the cemetery in Gabriella, a western replica town built to stage historic-gunfight reenactments and serve as a set for movie productions. Diamond lives and works in the remote settlement with his friend Larry Iams, a Vietnam veteran who was hospitalized by the VA in November 2021 following a suicide attempt.
Brandon Kapelow

A sunrise reflected in the windows at Dave Moller’s house outside of Alma, N.M. When Moller ended his own life, he left his treasured home and belongings to his friend Cresta.
Brandon Kapelow
Seniors especially feel the sting of loneliness. At the southern end of Catron County sits the Glenwood Senior Center, one of the few places left for older residents to gather. “They were going to shut down all the senior centers in Catron County, which, unfortunately, would have probably increased our suicide rate,” says Amy Whetham, the center’s supervisor. “These seniors, it’s the only thing they have.” Whetham has lost two family members to suicide and has struggled with several attempts through the years; she knows some of her colleagues have too, but nobody talks about it. “They’re older, and that’s how they were raised,” Whetham says. “You don’t talk about this stuff.”
Throughout the course of this project, residents kept telling me that it was easier to share their stories with a stranger than with members of their own community. I spoke with people of different ages and walks of life—from parents to police officers, teenage students to health care providers and county clerks—and despite every demographic being touched by suicide, most people hadn’t discussed it in a while. I was the one who kept having to end the conversation, as if they felt it might be a long time before they got the opportunity to talk about it again.
But there are signs of healing, too. Ron had always been private about his suicide attempt. But in December 2021, nearly two years after his life-altering crisis, he felt something inside him shift. He was ready to talk. He visited his neighbor Craig Lang, an EMT, to thank him for finding him, praying for him, and saving him that day. Ron also tried tracking down the deputy sheriff who was present, but Lang told him that the man had retired shortly after the incident because he kept having nightmares; he later moved out of the county.

Hilda Kellar, 73, is the mayor of Reserve and owner of K&B Timberworks, one of the region’s few remaining industrial employers. She has lost two family members to suicide, including her father, who struggled with chronic pain after an incident with falling timber. Her own struggles with physical pain gave her empathy. “My dad was ready to go, and I don’t judge him for it because I know how I have felt with that pain,” she says. “A few years back, I got back surgery … I was hurting so bad that I used to pray for God to take me. I also understand that you can survive it. So I know not to give up.”
Brandon Kapelow

Vicki Shriver, 64, the Reserve district EMS medical chief, and her husband Mike Shriver, 70, a pastor and retired state policeman, have both witnessed the shortcomings in their community’s response to mental health crises. “The public still needs people to be able to respond and be a neighbor,” Vicki says. “We take steps to care for ourselves to survive, honestly, because services have disintegrated.”
Brandon Kapelow

Firearms on display at a local gun show. In 1994, the Catron county commission voted unanimously to pass a nonbinding resolution stating that every household should possess a firearm and ammunition for the purpose of home defense. In 2019, the county joined a national movement of so-called “Second Amendment Sanctuaries,” where county commissioners and sheriff’s departments agree not to enforce gun-safety laws.
Brandon Kapelow

Reflections off Quemado Lake, near 19-year-old Hunter Gossett’s childhood home. “I was raised not to show emotion. If I cried, I was called a little bitch,” he says. “But luckily, I’ve learned that it’s OK to express emotion and not be OK sometimes. Try to always be OK, and you’re going to crumble.”
Brandon Kapelow

The road to Sunflower Mesa, where a local teen attempted suicide in 2002. Some attempt survivors, like Amy Whetham, supervisor of the Glenwood Senior Center, experience a change in perspective. “I started being more open about being bipolar, which seemed to help a lot,” she says. “Growing up, I didn’t want to talk to anybody. But it’s part of who I am. There’s nothing to be ashamed about. I know that I do want to live. I’m not ready to go anywhere yet.”
Brandon Kapelow
Ron now spends his days working the ranch with his wife and children, wondering why he was spared. He says that despite lingering feelings of regret, he ends each day filled with gratitude for being alive, for getting to enjoy more moments with his grandkids. “It would have fragmented my family, so maybe that’s why God let me live,” he says. He leans back into the seat of his truck and looks out toward the rolling cattle pastures. “Maybe just me talking to you is some of what it is. Maybe somehow I have kept somebody else from doing this. Maybe that’s what this is all about.”
If you or someone you know may be experiencing a mental-health crisis or contemplating suicide, call or text 988. In emergencies, call 911, or seek care from a local hospital or mental-health provider.
More Must-Read Stories From TIME
[ad_2]
Source link


[ad_1]
Pfizer-BioNTech announced that they now have the first human data hinting at how effective the new Omicron booster might be. The updated bivalent vaccine targets both the original SARS-CoV-2 strain and the currently circulating Omicron BA.4/5 variants and is authorized for use in Americans age 12 and older (and soon for ages 5 and older in a kid-sized 10 mcg dose, pending sign-off from the U.S. Centers for Disease Control and Prevention). That authorization was granted based on safety and efficacy studies in animals and data from a different vaccine targeting BA.1.
In the first results from human studies—which were announced by press release on Oct. 13 and not yet published in full—Pfizer-BioNTech reports that 40 people ages 18 to 55 who were boosted with the bivalent shot produced higher levels of virus-fighting antibodies against Omicron BA.4/5 seven days later compared to their starting levels. Among people 55 and older, those who received the Omicron booster generated higher levels of Omicron antibodies compared to those boosted with the original vaccine. That people produced more Omicron-specific antibodies after the booster is encouraging, especially since people in the study hadn’t been boosted for 11 months, on average, before receiving the bivalent vaccine. The companies did not provide a more detailed breakdown of the difference in the levels in their press release, but more data are expected in a few weeks.
The results are the first from an ongoing study involving more than 900 people 12 years and older who are receiving the Omicron booster at one of two doses: 30 mcg or 60 mcg. Everyone in the study has been boosted at least once with the original vaccine (which means they received at least three doses of the original shot). Their immune responses will be compared to those from people who have previously received two booster shots, or four doses, of the original vaccine. The FDA authorized the booster at the 30 mcg dose, but the trial will investigate whether the higher dose would provide additional protection. The companies plan to continue studying the Omicron BA.4/5 bivalent booster in younger children as well.
More Must-Read Stories From TIME
[ad_2]
Source link


[ad_1]
Teva Pharmaceutical Industries Ltd.’s shortage of Adderall is expected to last through March, longer than the two to three months the company said last week, according to U.S. regulators.
The popular treatment for attention-deficit/hyperactivity disorder has been in short supply since at least August, leaving people racing to fill prescriptions and find pharmacies with the elusive medication in stock. Demand for the drug is at an all-time high, and Teva sells more Adderall in the U.S. than any other drug company.
Teva “is experiencing ongoing intermittent manufacturing delays,” the FDA said on its website on Wednesday. While other companies are producing the drug, “there is not sufficient supply to continue to meet U.S. market demand through those producers.”
Read More: For Some Women With ADHD, TikTok Is the First Place They Felt Heard
Teva spokesperson Kelley Dougherty said that an earlier labor shortage at the company, which has since been resolved, combined with rising demand for the drug and manufacturing limits set by the U.S. Drug Enforcement Administration contributed to the shortage.
“We are working closely with our manufacturing facility and the DEA to see what additional volume we may be able to support in the future,” Dougherty said.
Five doses of Teva’s generic immediate-release Adderall are on backorder, with recovery expected in March, including the most popular 10mg, 20mg, and 30mg pills, according to the FDA. Most of Teva’s branded immediate-release formulations are available, but the 10mg tablets are also on backorder, with recovery expected this month.
Nine companies total have had trouble supplying Adderall recently.
The FDA lists three companies in addition to Teva with shortages—Epic Pharma LLC, Rhodes Pharmaceuticals LP (a subsidiary of Purdue Pharma LP) and SpecGX LLC (a subsidiary of Mallinckrodt Plc). In addition, the University of Utah’s Drug Information Service, which tracks drug shortages, reported last week that Amneal Pharmaceuticals Inc., Camber Pharmaceuticals Inc, Novartis AG’s Sandoz unit, Par Pharmaceutical (part of Endo International Plc), and Sun Pharmaceutical Industries Ltd., were having trouble supplying the drug.
More Must-Read Stories From TIME
[ad_2]
Source link


[ad_1]
Five months after the Democratic nominee in one of the nation’s most competitive Senate races suffered a stroke, there’s still a lot to learn about his recovery.
In the final weeks of the Pennsylvania Senate campaign, a key Republican attack against the state’s lieutenant governor, John Fetterman, has centered on his use of closed-captioning technology, which translates audio into text on a screen in real-time. He relied on the technology during an interview conducted Friday with NBC News, his first in-person, on-camera sit-down since his stroke in May.
“I sometimes will hear things in a way that’s not perfectly clear,” Fetterman said. “So I use captioning so I’m able to see what you’re saying.”
Fetterman also plans to use closed captioning for his upcoming debate with opponent Dr. Mehmet Oz, which is raising questions about Fetterman’s recovery.
Here’s we know so far.
Fetterman suffered a stroke in May, just before winning Pennsylvania’s Democratic primary for Senate. In June, his campaign released a letter from his cardiologist that said that “he should be able to campaign and serve in the U.S. Senate without a problem.” He has not released information from his medical team since then.
Fetterman said earlier this year that his stroke was caused by a clot. The type of stroke in which a blood clot blocks blood flow to the brain is called an ischemic stroke—the most common kind of stroke and one of the leading causes of disability in America, according to a February report from the American Heart Association. Ischemic strokes can cause a variety of long-term conditions depending on which part of the brain connects to the clogged artery. According to Johns Hopkins Medicine, a stroke in the left hemisphere of the cerebrum can cause aphasia: difficulty finding the right words or understanding what others are saying, or both.
Fetterman’s campaign said in June that he did not have aphasia, and his communications director Joe Calvello told TIME in October that’s still the case. Calvello did not respond to a follow-up question about the differences between that condition and Fetterman’s.
Fetterman’s need to use closed-captioning technology mirrors some of the challenges faced by the estimated one-third of stroke survivors dealing with aphasia. Some aphasia patients might struggle to speak in complete sentences, while others might use incorrect words. During the 32-minute NBC interview, Fetterman mispronounced and confused several words before correcting himself. He often paused to read questions before answering. He repeatedly dodged inquiries about why he will not release his complete medical records.
Maria Town, the president and CEO of the American Association of People with Disabilities, says Fetterman’s use of caption technology doesn’t mean he wouldn’t be able to do the job of being a Senator. “People use captions all the time,” Town says. “It doesn’t have anything to do with with competence.”
“Concepts like competency, or fitness—these are extremely flawed concepts for many marginalized communities, including people with disabilities,” she added.
Dr. Kevin Sheth, the founding chief of the Division of Neurocritical Care and Emergency Neurology at the Yale School of Medicine, also says that just because Fetterman is experiencing difficulties with speech, that doesn’t mean he is having other cognitive issues. “If you have a blockage in the blood vessels that supplies the part of the brain that plays an influential role in language, then you’re going to have trouble with language,” Sheth says. “If it’s the parts of your brain that control your strength and coordination in your limbs, then you’re going to have weakness or paralysis. The deficits that you have depend on the part of the brain that’s downstream from where the blockage in the blood supply was.”
In his NBC interview, Fetterman blamed his challenges on “auditory processing issues” and indicated that he struggled to understand what he was hearing shortly after his stroke, but that his ability to do so has improved since then. Captioning, Fetterman said, helps him be precise.
Oz’s campaign manager suggested Fetterman wouldn’t be able to use closed-captioning on the Senate floor. Asked by NBC if he would need similar accommodations in the Senate, Fetterman replied, “I don’t think it’s going to have an impact. I feel like I’m going to get better and better every day and by January, I’m going to be much better and Dr. Oz is still going to be a fraud.”
“As we’ve said over and over again, John is healthy and he also still has a lingering auditory processing issue that his doctors expect will go away,” Calvello wrote in a statement Thursday. “The whole point of the NBC News interview was to show how John is conducting this campaign and doing his interviews.”
Scientists and doctors are still working to understand stroke recovery, which varies considerably from patient to patient. Outcomes can range from full recovery to permanent disability, and many factors—such as physical therapy, rehabilitation, and lifestyle changes—can affect the process. But in general, recovery tends to follow a particular pattern. “If I draw a graph, I would draw one of those curves where you get steep recovery early, and then over time, the slope can still be there, but it starts to flatten out,” says Sheth. “The recovery between month 14 and 15 might be pretty small, whereas the recovery between two weeks and four weeks might be much bigger.”
When it comes to aphasia in particular, some research indicates that the bulk of improvement happens in the first three months, though survivors can continue to see slow improvement for years, just as they can with all symptoms after a stroke. “If a person at five months has a certain amount of deficits, it’s not like those deficits are going to disappear the next week,” Sheth says. “It’s gonna take some time.”
More Must-Read Stories From TIME
[ad_2]
Source link


[ad_1]
Public health data signals a genuine crisis in adolescent mental health: rising rates of anxiety, depression, and hopelessness. But as we worry about tweens and teens who are struggling, we can’t ignore another mounting toll—the burdens that are shouldered by their friends and peers in an “always on” world.
We have studied teens and tech for over a decade. Still, what we learned in our most recent study stopped us in our tracks. We collected perspectives from more than 3,500 teens on the best and trickiest parts of growing up in a networked world, and we co-interpreted these perspectives alongside other teens who helped us make sense of what we were hearing.
Here’s what they told us: Their networks are ever-expanding, in no small part because there’s a sense that being “nice” means by default accepting follow requests from acquaintances and friends-of-friends. We often tell teens not to connect with strangers, yet we overlook the complexities of staying connected to anyone and everyone they meet. Teens tell us, “I don’t want to hurt anybody’s feelings if I can’t stay in touch with them.” And it’s not just staying connected—it’s keeping up with what others post, too.
Evidence from both human beings and primates indicates that we have a natural capacity to limit our social networks. Today, apps like Instagram, Facebook, and Twitter make it easier to keep up more connections at a lower cost in terms of time investment. But it may be that the very architecture of our brains is the reason we have defaulted to the same average network size throughout history. Perhaps you’ve heard of “Dunbar’s number,” representing the number of individuals with whom humans can maintain stable relationships. Prepare yourself: it’s (only) 150! Social media platforms thus make it technically possible to “maintain” more relationships than we are historically actually wired to track and manage. The result is an overwhelming water hose of social information. It’s especially intense for adolescents whose developmental sensitivities drive them to care deeply about what their peers are doing and thinking.
How can parents and adults help? It’s tempting to criticize teens’ sensitivity to social pulls or to roll our eyes when they obsess over their friends’ locations on Snapchat’s Snap Map. But these reactions give teens a sense that we don’t “get it,” and they dead-end dialogue rather than opening up conversations teens need.
Read More: Instagram Is Doing Grave Harm to Our Generation. We Need Help to Stop It
We’ve seen firsthand that combining genuine curiosity with empathy and validation is a magic formula. Ask questions like, “What is it like to be able to see where your friends are all the time? Are there times when it’s helpful? Are there times when it’s hard?”, and then follow-up with validating statements such as, “I can see how that helps you stay connected, but also how it could make you feel left out.” When we take this tack, teens keep talking—and we keep learning. They’re also more inclined to actually listen to advice we have to share. What’s more, asking teens genuine questions creates space for them to reflect on their connected lives. This builds a kind of metacognitive awareness, which the fast-pace and clever design features of apps otherwise undermine at nearly every turn.
Teens tell us about significant stresses that come with trying to be a “good friend” in the age of social media, too. Friendship requires both public and behind-the-scenes support. Even before a social media post is made public, close friends can be pulled into photo selection, editing, and final vetting. Once posts appear, friends are expected to step up—and fast. Liking posts is the bare minimum. A seventeen-year-old recounted how liking a friend’s post immediately triggered a direct message asking her why she hadn’t commented yet. “Then I have to comment like three times…,” she explained, “And I get really nervous about it too, because I have to think of something quick, and it has to be something really good.”
Another pressure is responding the ‘right’ way and in the ‘right’ amount of time, which differs from one relationship to another. Read receipts are implicated here; they signal that a message has been “Read.” To many teens, the time between a message being Read and reciprocated matters a lot. Replying too quickly can be seen as over-eager, especially when the friendship is new or not close. But when it’s a close friend, too long a lag can be hurtful. One teen told us, “If I don’t stay connected, the friendship will fall apart.” Anxious second- and third-guessing of text wording and response times has become a routine part of teen courtship, too.
Teens also told us about the burden of bearing constant witness to peers’ mental health struggles on public display via Instagram stories, TikTok videos, disappearing Snaps, and more. Certainly, the “highlight reel” quality of social media posts—everyone is apparently living their best life—can be hard for some teens. But there’s a kind of emotional whiplash that comes as teens see peers’ cutest pics interspersed with cries for help.
Appropriately, the stakes feel high. A fourteen year old told us, “My biggest worry is that I don’t have enough contact with friends who are struggling…I don’t want my friends to do something bad just because I didn’t respond in time to stop them from harming themselves or worse.” This is a big weight on young shoulders, and a sentiment we’ve heard on repeat.
Vivid stories clarified how these dynamics can play out. When fifteen-year-old Aly saw her classmate Jaylen’s Snapchat posts hint at suicidal thinking, she started to worry. But she struggled to interpret the messages and figure out what to do. Then, Jaylen’s posts got more explicit and Aly’s worry shifted to panic. She grappled with a question we heard other teens voice: What should you do (and who should you tell) if a peer’s social media posts seem alarming?
The challenge of interpreting social media posts—and speaking up—feels all the more relevant in a time when mass shootings are recurring events and digital evidence of threats is unearthed after the fact. In some cases, the poster’s message is clear and so too are their intentions to cause violence. But much of what teens see in their everyday lives falls into a kind of grey area: They don’t always know what is a joke versus a real threat.
How can adults help teens manage this particular burden? We need to first teach teens to pay attention to red flag feelings—and even yellow flag feelings: the gut sense that something is (or might be) off. We then need to talk to teens about what they should do when they see such posts, which starts with looping in others. Have teens identify a few trusted adults who they can turn to for help. In Aly’s case, she told her mom, and her mom contacted Jaylen’s parent. They were already at the emergency room, but Jaylen’s mom had no idea that Jaylen was posting about his distress.
Above all, encourage teens not to just scroll on or struggle in silence. Especially for kind and sensitive kids, the burden can be heavy. They shouldn’t bear this load alone. Nor should they put aside their own needs for sleep, joy, and other essentials. So teens who are supporting fragile friends may need guidance in setting boundaries that respect their friendships and themselves. How do you tell someone that you care and that you’re not available around the clock? Adults can help teens find kind but self-protective language that communicates when they need to disconnect. Encouraging teens to help their friends access other sources of support (like school counselors) is also key.
The qualities that make or break friendships are actually the same as they’ve always been: mutual sharing of joys and sorrows, a give and take of validation and support, and an ability to weather and resolve conflicts. But technologies have transformed how friendships play out. Social media intensifies the burdens that come along with being a good friend. Too often, these dynamics hit teens hard in ways that are lost on adults. We need that to change.
More Must-Read Stories From TIME
[ad_2]
Source link