Dani Yuengling of Conway, South Carolina, knew she had to follow up after a mammogram found a lump. Her mom had died of breast cancer. But she had no idea how expensive the biopsy would be.
Gavin McIntyre for KHN
hide caption
toggle caption
Gavin McIntyre for KHN
Dani Yuengling of Conway, South Carolina, knew she had to follow up after a mammogram found a lump. Her mom had died of breast cancer. But she had no idea how expensive the biopsy would be.
Gavin McIntyre for KHN
When Dani Yuengling felt a lump in her right breast last summer, she tried to ignore it.
She was 35, the same age her mother had been when she received a breast cancer diagnosis in 1997. The disease eventually killed Yuengling’s mom in 2017.
“It was the hardest experience, seeing her suffer,” said Yuengling, who lives in Conway, South Carolina.
After a mammogram confirmed the lump needed further investigation, Yuengling scheduled a breast biopsy for Valentine’s Day this year at Grand Strand Medical Center in Myrtle Beach.
Among many concerns she had ahead of that appointment — the first being a potential cancer diagnosis — Yuengling needed to know how much the biopsy would cost. She has a $6,000 annual deductible — the amount her health plan requires she pay before its contribution kicks in — and she wasn’t close to hitting that. Whatever the procedure cost, Yuengling knew she’d be on the hook for most of it.
But the hospital wouldn’t give her a price. She was told her providers wouldn’t know what type of biopsy needle they needed until the procedure was underway and that would impact the price.
The hospital’s online “Patient Payment Estimator” showed that an uninsured patient would owe about $1,400 for the procedure.
“That’s fine. No big deal,” she thought to herself, confident it would be cheaper for her because she did have insurance. A Google search indicated it could be closer to $3,000, but Yuengling thought that price seemed reasonable, too. She wasn’t fretting too much about money as she underwent the procedure.
It soon brought the good news that she didn’t have cancer.
Then the bill came.
The patient: Dani Yuengling, now 36, who is covered by Cigna through her employer, a human resources contractor for the Mayo Clinic.
Medical service: An ultrasound-guided breast biopsy.
Service provider: Grand Strand Medical Center, a 403-bed, for-profit hospital in Myrtle Beach, South Carolina. It is one of 182 hospitals owned by Nashville-based HCA Healthcare, which generated $58.7 billion in revenue last year.
Total bill: $17,979 for the procedure, including lab work, pharmacy charges, and sterile supplies. Cigna’s in-network negotiated rate was $8,424.14, of which the insurance company paid the hospital $3,254.47. Yuengling was billed $5,169.67, the balance of her deductible.
What gives: It’s not uncommon for uninsured patients — or any patient willing to pay a cash price — to be charged far less for a procedure than patients with health insurance. For the nearly 30% of American workers with high-deductible plans, like Yuengling, that means using insurance can lead to a far bigger expense than if they had been uninsured or just pulled out a credit card to pay in advance.
Ge Bai, an associate professor at Johns Hopkins Bloomberg School of Public Health, recently published research on this topic and said hospitals in the U.S. often set their cash prices lower than the prices they charge to treat commercially insured patients.
“We can very confidently say this is very common,” said Bai, who advised that all patients, regardless of their insurance status, inquire about the cash price before undergoing a procedure. “It should be a norm.”
Grand Strand charged Yuengling’s insurance an extraordinarily high price for her procedure. By comparison, according to the federal government’s website, Medicare patients who need an ultrasound-guided biopsy similar to the one Yuengling received would pay only about $300 — their required 20% coinsurance for outpatient care. Medicare would pay the hospital the remainder of the bill, about $1,200. The hospital expected more than five times the Medicare price from Yuengling and her insurer.
Patients in Conway with private health insurance who are treated at other hospitals also typically are charged less than what Yuengling paid for the same procedure — on average about $3,500, according to Fair Health Consumer, an organization that analyzes health insurance claims.
And uninsured patients who pay cash prices and need an ultrasound-guided breast biopsy at the nearby Conway Medical Center are likely to owe even less — about $2,100, according to Allyson Floyd, a spokesperson for the hospital.
Meanwhile, Grand Strand Medical Center spokesperson Caroline Preusser blamed “a glitch” involving the hospital’s online calculator for the inaccurate information Yuengling received and said the correct estimate for the cash price for a breast biopsy at the hospital is between $8,000 and $11,500 “depending on the exact procedure and equipment used.”
The hospital removed certain procedures from the payment estimator until they can be corrected, Preusser wrote. She did not say how long that would take.
Resolution: Yuengling tried disputing the charges with the hospital. She called the billing department and was offered a 36% discount, lowering the amount she needed to pay to $3,306.29. Grand Strand Medical Center allows patients to set up payment plans, but Yuengling decided to charge the full amount to a credit card because she wanted the whole thing to go away.
“I could not sleep. It was driving me crazy. I was having migraines. I was sick to my stomach,” she said. “I hate having debt. I didn’t want to think about it. Obviously, that didn’t work because I’m still thinking about it.”
She said she requested on multiple occasions to speak to the hospital’s patient advocate and was eventually connected with an outside company, Parallon, which conducted an audit of her bill. She eventually received a letter dated May 26 from the hospital’s Revenue Integrity Department. It stated: “After a review of the charges in question and your medical record, the following was identified; The charges on your account were appropriate.”
“I don’t know why I actually expected a different outcome,” she said.
The hospital has requested that Yuengling return for a follow-up appointment related to the biopsy. She has refused.
Harlow Sumerford, a spokesperson for HCA Healthcare, told KHN in an email that the hospital system apologizes for any confusion caused by the payment estimator “and we are working to fix the issue.”
Dani Yuengling of Conway, South Carolina, had a $6,000 annual deductible on her health plan. Because of that, she was on the hook for a big share of the costly biopsy.
Gavin McIntyre for KHN
hide caption
toggle caption
Gavin McIntyre for KHN
Dani Yuengling of Conway, South Carolina, had a $6,000 annual deductible on her health plan. Because of that, she was on the hook for a big share of the costly biopsy.
Gavin McIntyre for KHN
The takeaway: With a family history of breast cancer, Yuengling was right to follow up with her doctor after feeling a lump. After failing to get a clear answer on her costs from Grand Strand Medical Center, she could have taken an additional step to explore what other hospitals in the area charge. Although her physician referred her to Grand Strand, she was not obligated to use that hospital. She could have saved a significant amount of money by opting to undergo the procedure elsewhere.
Furthermore, patients like Yuengling who have a high-deductible insurance plan should consider paying cash prices for certain procedures and not involving their insurance company at all.
Jacqueline Fox, a health care attorney and a professor at the University of South Carolina School of Law, said she isn’t aware of any law that would prohibit a patient from doing that. After all, she pointed out, patients with health insurance pay cash prices for prescription medications all the time. It stands to reason they could do the same for medical procedures.
But some facilities make this difficult. Grand Strand Medical Center, for example, offers “self-pay” patients an “uninsured discount,” but that discount is limited to people who have “no third party payer source of payment or do not qualify for Medicaid, Charity or any other discount program the facility offers,” according to the hospital’s website. Only patients confirmed to have no health insurance are offered information about the discount.
In some cases, paying a cash price for a procedure might not make financial sense in the long run because none of it would be applied toward the deductible. Patients might save money on one procedure but end up paying their full deductible if unexpected medical expenses mount later during the calendar year.
Insured patients should reach out to their health plan for a good-faith estimate before a procedure. Under the No Surprises Act, health plans are supposed to give members an idea of their total out-of-pocket costs upon request. Ask for an “Advanced Explanation of Benefits,” said Sabrina Corlette, a research professor at the Georgetown University McCourt School of Public Policy, though she points out this part of the law isn’t being enforced yet.
The No Surprises Act also allows patients to file complaints with the federal government regarding their medical bills — whether or not they carry health insurance.
Yuengling filed her complaint in June.
Stephanie O’Neill contributed the audio portrait with this article.
Bill of the Month is a crowdsourced investigation by KHN and NPR that dissects and explains medical bills. Do you have an interesting medical bill you want to share with us? Tell us about it!
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. It is an editorially independent major operating program of KFF (Kaiser Family Foundation).
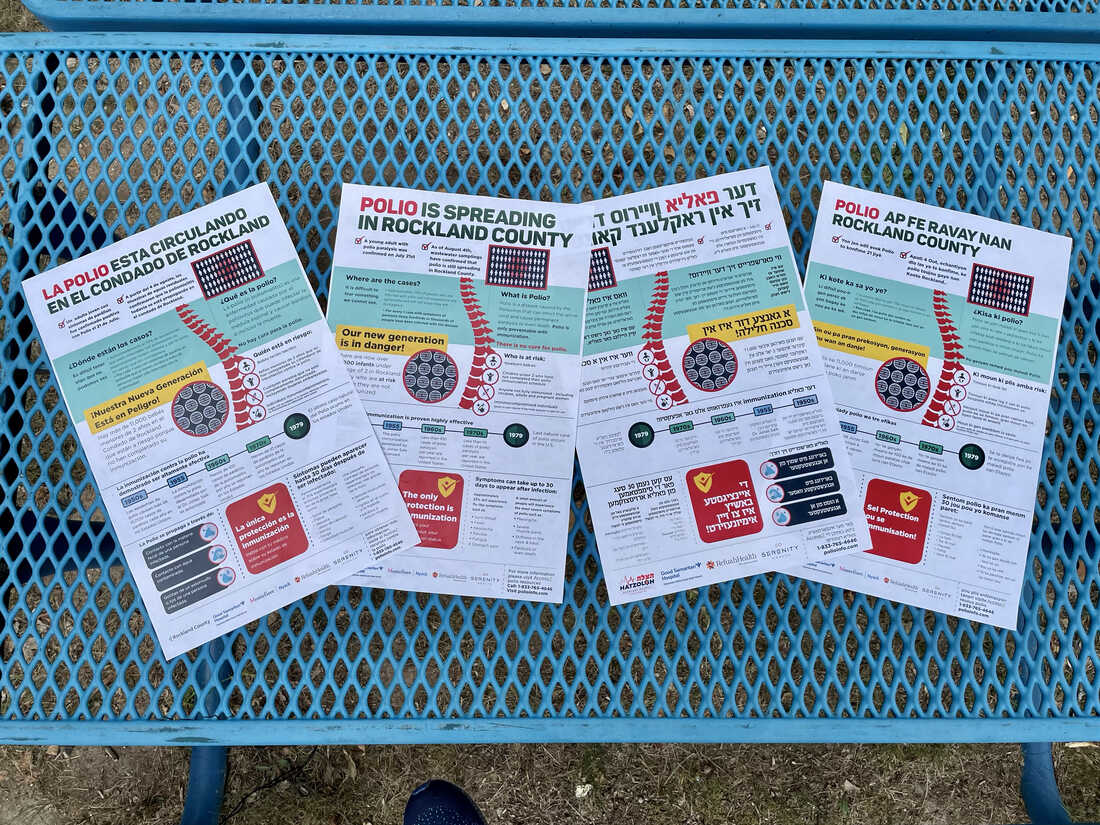
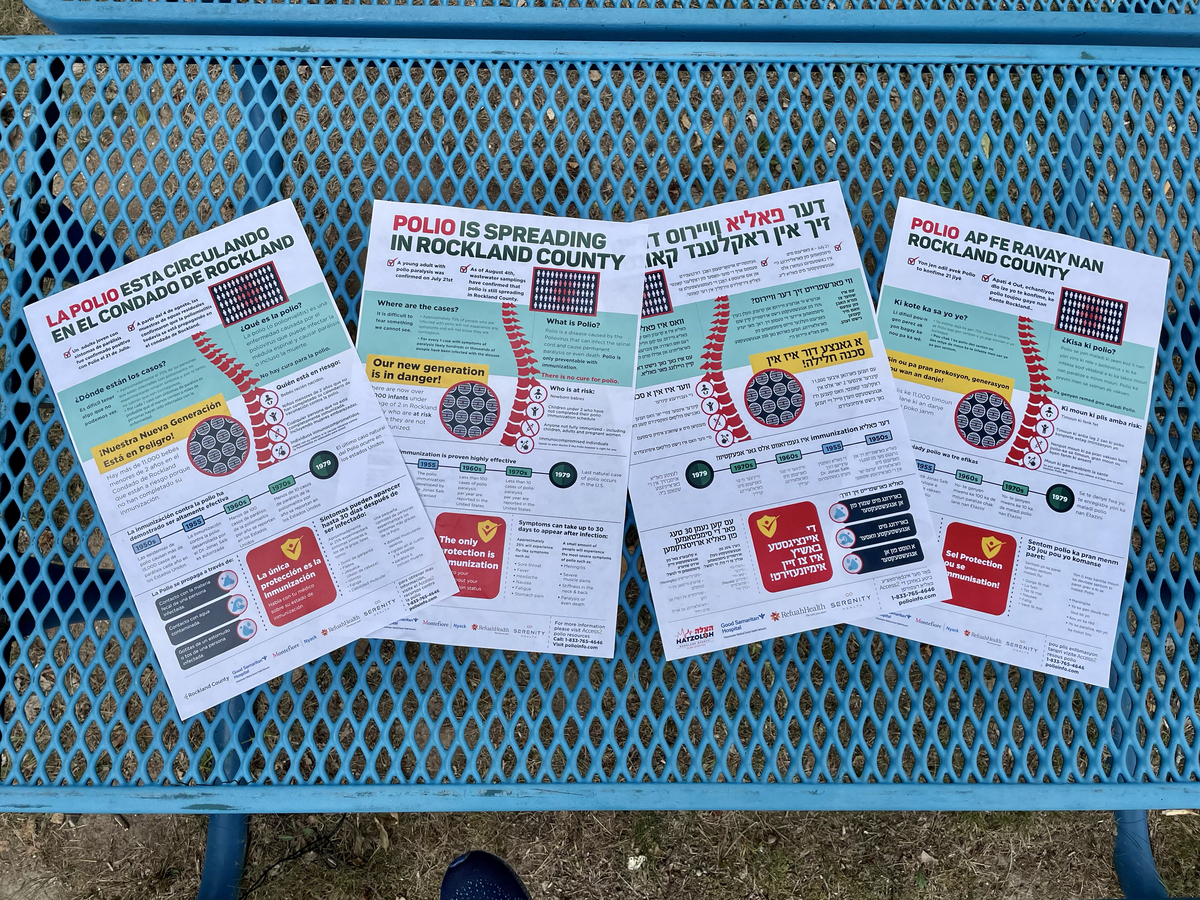
This carefully-worded and designed infographic from Rockland County, NY describes — in English, Spanish, Haitian Creole, and Yiddish — what polio is and that immunization is the best way to protect yourself and others.
Ari Daniel for NPR
hide caption
toggle caption
Ari Daniel for NPR
This carefully-worded and designed infographic from Rockland County, NY describes — in English, Spanish, Haitian Creole, and Yiddish — what polio is and that immunization is the best way to protect yourself and others.
Ari Daniel for NPR
Polio is the disease most people thought we had put behind us here in the United States. But earlier this summer, an individual in Rockland County, N.Y., contracted the virus likely from exposure in this country, and ended up paralyzed.
The last time there was community transmission of polio in the U.S. was 1979. The Americas were declared polio free in 1994. Though it’s just one case of paralysis at the moment, public health officials — both locally and nationally — are taking the news very seriously.
Wastewater testing and genetic sequencing have shown the virus has been quietly circulating in a couple New York counties since at least May. And it recently was detected in New York City’s wastewater. “Even a single case of paralytic polio represents a public health emergency in the United States,” the Centers for Disease Control and Prevention declared in a recent report.
Low vaccination rates in Rockland county mean there’s a risk of more paralytic cases in that community, the report said. The challenges that health officials are facing while managing the local response in New York may indicate where other spots in the country could soon be headed.
“Rockland County is basically New York City,” says Perry Halkitis, dean of the School of Public Health at Rutgers University. “New York City is basically New Jersey. Rockland County is basically Connecticut.” Because people travel so much, diseases like polio can spread quickly, he explains. “Are there probably dozens, if not hundreds, if not more cases of undetected polio in our population? Probably. Are we catching them? Probably not.”
And health officials have to tackle this outbreak in a moment of rising wariness towards public health fueled by the COVID crisis.
A feeling of dread
The news about the paralytic case circulated amongst those in local government before it was announced to the public. Mona Montal — chief of staff for the town of Ramapo in Rockland county — remembers what went through her head: “Here we go again.” She was, of course, thinking of the grueling last two plus years of combatting COVID. “Do I as an individual, and do we collectively, as a county and as a community, have the strength to go through this again?,” she wondered.
Shoshana Bernstein and Mona Montal have joined forces in Rockland County to become a vital conduit between official public health messaging and the hearts and minds of their neighbors.
Ari Daniel for NPR
hide caption
toggle caption
Ari Daniel for NPR
Shoshana Bernstein and Mona Montal have joined forces in Rockland County to become a vital conduit between official public health messaging and the hearts and minds of their neighbors.
Ari Daniel for NPR
And polio, with its possibility of paralysis, is an especially terrifying disease. “Polio cannot be cured,” Montal explains. “And once it’s paralytic polio, you’re paralyzed. Plain and simple.”
Before the vaccine was rolled out across the U.S., paralysis and children in braces and wheelchairs were among the haunting images of outbreaks from the 1940s and 50s. In fact, Montal was told stories of her own family members who died or were paralyzed by the disease.
During COVID, she worked on the county’s COVID vaccine information campaign, alongside Rockland County resident Shoshana Bernstein, an independent health communicator. The news of paralytic polio had Bernstein in knots. “I’ll check my phone about seven times a night,” she says. “I wake up like, ‘Oh my God, is there another case?'”
A very small percentage of people with polio become paralyzed. Most of the time, there are no symptoms at all. Which is why, in public health, just one case of paralytic polio constitutes an outbreak — the tip of the iceberg.
“It’s very difficult to predict how many people, but it’s definitely a number of individuals that would have to be actively transmitting,” says Dr. Irina Gelman, Commissioner of Health, Orange County, which is next door to Rockland. “Clearly a confirmed case of polio in the United States is major news.”
When Rockland and Orange Counties started testing the wastewater for polio, samples going back to May were positive for polio. Then, sequencing the virus’ genetic material surfaced something else that was unsettling.
“There are multiple strains, so they are different,” says Gelman, “meaning we do know that it’s more than one individual” who is shedding polio virus. In other words, the outbreak isn’t contained.
This treatment facility in Rockland County is ground zero for where the polio virus was first detected in wastewater within New York State.
Ari Daniel for NPR
hide caption
toggle caption
Ari Daniel for NPR
This treatment facility in Rockland County is ground zero for where the polio virus was first detected in wastewater within New York State.
Ari Daniel for NPR
The risk of low vaccination rates
Falling vaccination rates are a big part of the problem, in the U.S. and abroad. During the pandemic, many children missed shots and vaccine services were disrupted, the CDC notes in its report on the Rockland polio case. Nationally, by age two, nearly 93% of infants born during 2017-2018 were vaccinated for polio. But according to the New York State Immunization Information System, vaccination coverage among infants and children less than 24 months living in Rockland County was 60.3% in August 2022. In some communities, coverage was as low as 37.3%.
“I mean, to put it bluntly, it’s just disappointing at this point that we are still here,” Gelman says. “This is a vaccine-preventable disease. And had everyone just been up-to-date on their vaccination, we would have continued to report it as being eradicated.”
Here’s how authorities think the virus got here:
A person came to New York State infected with a strain of polio which is connected to samples found in the wastewater of Israel and the UK. The person didn’t realize they had polio: They didn’t have symptoms, or they were mild or generic. Then, because vaccination levels are low in some communities in New York State, the virus started spreading, eventually causing paralysis in a person in Rockland. The virus then continued to fan out, since Rockland and Orange Counties have some of the lowest polio vaccination rates for young kids in the country.
“It’s a multitude of reasons spread across a multitude of demographics,” says Bernstein. “There’s no one single group that is not vaccinated.” This is true not just of these communities in and around New York City.
“We have a large number of…populations who are choosing not to vaccinate [their children],” says Halkitis. “And so it is a reality across our country. We know from territory to territory, from borough to borough, from neighborhood to neighborhood, there’s wide variation right now.”
That is, although polio has only been detected in these few places in New York State so far, Halkitis warns it’s likely to spread to other places near and far with pockets of low vaccination.
Orange County Commissioner of Health Dr. Irina Gelman is concerned about the outbreak. “Clearly a confirmed case of polio in the United States is major news,” she says.
Ari Daniel for NPR
hide caption
toggle caption
Ari Daniel for NPR
Orange County Commissioner of Health Dr. Irina Gelman is concerned about the outbreak. “Clearly a confirmed case of polio in the United States is major news,” she says.
Ari Daniel for NPR
Tackling vaccine hesitancy
If polio does show up in other places in the U.S., they are likely face some of the same challenges Rockland and Orange Counties have encountered in reaching communities that are under-vaccinated.
Bernstein explains that COVID and all the talk of vaccinations just made everyone tired and confused in Rockland County. She’s a member of the large ultra-Orthodox Jewish population here, some of whom, she says, choose to live a more insular lifestyle.
“Social and secular media is not really something that’s brought in,” Bernstein says. “So it’s a lot of word of mouth,” which, she acknowledges, makes some within her community vulnerable to anti-vaccine messaging. “We always say it’s extremely easy to instill fear and extremely difficult to undo it,” says Bernstein.
The county is a mosaic of people where vaccination rates are also low, including members of the Haitian and Latino communities. “I think any press release from the CDC is just — no one’s even reading it,” Bernstein says.
So Bernstein and Montal have joined forces to become a vital conduit between all the official public health language and the hearts and minds of their neighbors. The duo helped initiate a large printed infographic, which is hot off the presses. There are four versions in English, Spanish, Haitian Creole, and Yiddish. Montal says it’s carefully worded.
“People have had PTSD with the word vaccination,” Montal explains. “So we’re immunizing, we’re not vaccinating. And that’s the messaging.”
The two women work with trusted community leaders, like rabbis and pastors, to get the word out. And they’ve asked the CDC for a letter they can show these leaders that supports them in that effort.
“My dream is that after this,” says Bernstein, “the CDC will actually have like a game plan of, ‘Okay, we’re using Rockland County as our model. And now we’re going to repeat that model across the country.'”
The Rockland County Department of Health has organized a variety of polio-only immunization clinics in different locations once or twice a week. Montal says, “We have to bring the immunizations to the people. We can’t expect the people to come to us.”
To that end, last Wednesday afternoon in Spring Valley, at a polio immunization clinic, a total of about 15 people stopped by over a couple hours. Brian Hastings drove two hours from Long Island for a shot. Dolores Thaxton, who’s 89 years old, was never vaccinated for polio and decided to roll up her sleeve.
This kind of outreach is a long-term effort, that may slowly pay off. Abigail Guerrero, a young mother from Ecuador who speaks very little English, came to the clinic for something else but saw the large infographic in Spanish taped up — the one that Bernstein and Montal helped make. This sign was her first encounter with the polio outbreak in her community and after reading it and learning about the disease, she decided to get immunized.
Back in Orange County, Commissioner of Health Dr. Irina Gelman says she’s a sound sleeper, because she doesn’t get much of it. She’s up at 3:30 every morning. The drumbeat of disease hasn’t let up since she began her job four years ago.
“We started with the measles outbreak,” she says. “And we’ve gradually progressed into COVID 19. And simultaneously, we are now dealing with monkeypox. And with now polio. It was officially eradicated, yes. It does pose a tremendous amount of concern.”
Call center specialist Michael Colluccio works on a team that answers 988 calls from people whose phones have area codes for the suburban Philadelphia region. If needed, Colluccio also can answer calls from other parts of the state or country, part of a system that makes sure someone is always available to talk.
Brett Sholtis/WITF
hide caption
toggle caption
Brett Sholtis/WITF
Call center specialist Michael Colluccio works on a team that answers 988 calls from people whose phones have area codes for the suburban Philadelphia region. If needed, Colluccio also can answer calls from other parts of the state or country, part of a system that makes sure someone is always available to talk.
Brett Sholtis/WITF
On a Friday evening at a call center in southeastern Pennsylvania, Michael Colluccio stirs his hot tea, puts on his headset, and starts up his computer. On the screen, calls are coming in to the suicide prevention lifeline from around the state.
The 38-year old Colluccio says he knows what it’s like to be on the other end of one of those calls.
“So I had a suicide attempt when I was about 10, 11 years old,” Colluccio says. “And we do get callers who are about that age, or quite young, and they are going through similar stressors.”
For people having a mental health crisis, calling 988 can be a life-saving decision. But what happens after you call depends on where you are. The new 988 system launched in mid-July, and one early estimate says calls went up 45% nationally during the first week.
With calls expected to increase more as people learn about the helpline, some call centers say there are limits to what they can accomplish without more local resources.
Colluccio says callers in this area — Bucks County, a suburb of Philadelphia — have access to more services than in many parts of the state. His job with the Family Service Association, which runs the hotline, sometimes involves connecting them with services such as homeless shelters, therapists or drug and alcohol counselors.
More than anything, his job is to listen.
‘If you did not pick up, I’d have killed myself’
Colluccio’s first call of the evening is from a woman who sounds panicked. Her partner has been using drugs and has started making violent threats.
He spends a lot more time listening than talking. He says by listening closely to what she has to say, he offers relief, validation and human connection.
When he does talk, he usually asks questions — gently searching for specific ways to help. In this case, his questions lead him to connect the caller with local domestic abuse services and a social worker.
One service he rarely turns to is 911. Part of the idea behind 988 is that it offers an alternative to involving police or an ambulance for a mental health crisis. He would typically use 911 only if someone was an immediate threat to themselves or others.
After talking with the woman for a half hour, Colluccio asks her a few key questions to determine whether she feels suicidal. Colluccio says this is an important step to make sure each caller is safe after they hang up.
What happens next is surprisingly common. At the start of the call it seemed like the woman wanted help for her partner. But when he asks her directly on a scale of one to five how suicidal she is, she says she’s a two or maybe a three — and she’s attempted suicide before.
Before they end the call, Colluccio asks her if she would like a call back tomorrow. She says yes, so he schedules one.
Colluccio has just enough time for a sip of tea when another call comes in. It’s a young man in college, overwhelmed by stress. They talk for over an hour.
This is a pretty typical evening.
“Sometimes it’s more of an immediate intervention because sometimes people call with pills in hand and are actively considering ending their lives,” Colluccio said. “There are people who have called and said, if you did not pick up, I’d have killed myself.”
He says that’s why having a national network of call centers works so well. There are more than 200 call centers like this one across the country. Calls are tied to area codes. If nobody picks up locally, the call gets kicked to somewhere else.
The promise is to always have someone pick up the phone.
Jayne Wildasin runs True North Wellness Services Crisis Intervention in Hanover, Pennsylvania. Because of limited resources in the area, sometimes call center workers do in-person visits, a job that is usually handled by mobile crisis teams.
Brett Sholtis/WITF
hide caption
toggle caption
Brett Sholtis/WITF
Jayne Wildasin runs True North Wellness Services Crisis Intervention in Hanover, Pennsylvania. Because of limited resources in the area, sometimes call center workers do in-person visits, a job that is usually handled by mobile crisis teams.
Brett Sholtis/WITF
Strained resources for in-person help
In some places, like Bucks County, there are options for callers who need more help than counselors can offer on the phone. Colluccio says he can even dispatch a mobile crew of mental health workers to visit someone at their home.
But that’s not the case everywhere. In Hanover, a small town a few hours west, the 988 call center doesn’t have that option.
Jayne Wildasin runs that center and says workers sometimes have to put down their headsets, get in their cars and go meet with people sometimes as far as an hour away.
“So right now if there’s a crisis at someone’s house we could potentially go there,” Wildasin says.
In rural Centre County, the local 988 call center relies on volunteers — mostly college students from Penn State University. Denise Herr McCann runs the operation and says that her team can call in mobile mental health experts, but there need to be more of them.
Plus there’s a gaping need for other mental health professionals to continue helping people once the crisis has passed.
“Sometimes those resources are other counseling services, and they don’t have capacity,” Herr McCann says. “People are calling, and providers are six weeks out if they’re lucky. That’s not any good.”
For decades, suicide prevention call centers have had to scrape together funding from local, state and federal sources. Now with the switch to 988, they have to meet new federal regulations, such as data collecting and licensure requirements, says Julie Dees, who oversees the call center in Bucks County. That all costs money.
“There are increased responsibilities that are being put on the call centers, but there’s really no additional funding being put on that,” Dees says.
It’s an issue around the U.S., according to a recent analysis from The Pew Charitable Trusts. The group notes that states are largely left to foot the bill for the change to 988 — and many of the call centers doing the actual work have been underfunded for years. It recommends that state policymakers evaluate funding needs to ensure that crisis services connected to 988 will be sustainable.
The Biden administration has dedicated $432 million toward building the capacity of local and backup call centers and providing associated services. But the expectation is that states will come up with the main funding streams.
The 2020 law enacting the 988 number also allows states to pass legislation to add a small fee to cell phone bills as a permanent source of funds for 988 and associated mental health services. So far, only four states have done so, and only two more have proposed legislation.
Pennsylvania is not one of those states, and doesn’t have any other funding plan implemented. That worries Kevin Boozel, who heads the County Commissioners Association of Pennsylvania.
“This is life or death,” Boozel says. “And you can’t halfway do it.”
He pointed out that Pennsylvania has decided to hold back on publicizing the new 988 number until next year. The fear is that too many calls could flood the system, and counties need more time to set up funding, hire workers and build capacity for things like those mobile crisis teams.
Challenges aside, In Centre County, Herr McCann emphasizes that calling the hotline works. In most cases, just talking with someone is enough to defuse a crisis.
“When they have someone who is empathetic and who listens, that connection helps them,” she said. That lets people know that “it isn’t hopeless. There is hope out there. There is help out there.”
A single-use syringe awaits to be filled with the Moderna COVID-19 vaccine. Moderna has sued rival drugmakers for patent infringement.
Rogelio V. Solis/AP
hide caption
toggle caption
Rogelio V. Solis/AP
A single-use syringe awaits to be filled with the Moderna COVID-19 vaccine. Moderna has sued rival drugmakers for patent infringement.
Rogelio V. Solis/AP
Vaccine maker Moderna announced Friday that it’s suing rival drugmakers Pfizer and BioNtech for patent infringement. The lawsuit alleges the two companies used certain key features of technology Moderna developed to make their COVID-19 vaccine. It argues that Pfizer and BioNtech’s vaccine infringes patents Moderna filed between 2010 and 2016 for its messenger RNA or mRNA technology.
All three companies’ COVID-19 vaccines used mRNA technology which is a new way to make vaccines. In the past, vaccines were generally made using parts of a virus, or inactivated virus, to stimulate an immune response. With mRNA technology, the vaccine uses messenger RNA created in a lab to send genetic instructions that teach our cells to make a protein or part of a protein that triggers an immune response.
In October 2020, Moderna pledged not to enforce its COVID-19 related patents while the pandemic was ongoing, according to a statement from the company. In March this year, it said it will stick to its commitment not to enforce its COVID-19 related patents in low and middle-income countries, but expects rival companies like Pfizer to respect its intellectual property.
Moderna is not seeking to remove the Pfizer and BioNTech vaccine from the market, but is seeking monetary damages.
Moderna is filing the lawsuits against Pfizer and BioNTech in the U.S. District Court in Massachusetts and the Regional Court of Düsseldorf in Germany.
A Pfizer spokesperson said in a statement the company has not yet fully reviewed the complaint but it is “confident in our intellectual property supporting the Pfizer/BioNTech vaccine and will vigorously defend against the allegations of the lawsuit.”
Physician Assistant Susan Eng-Na, right, administers a monkeypox vaccine during a vaccination clinic in New York. New cases are starting to decline in New York and some other U.S. cities.
Mary Altaffer/AP
hide caption
toggle caption
Mary Altaffer/AP
Physician Assistant Susan Eng-Na, right, administers a monkeypox vaccine during a vaccination clinic in New York. New cases are starting to decline in New York and some other U.S. cities.
Mary Altaffer/AP
More than three months into the U.S. monkeypox outbreak, there’s a new – and welcome – phrase coming from the lips of health officials who are steering the country’s response: cautious optimism.
The change in tone reflects early signs that rates of new infections are slowing in some of the major cities where the virus arrived early and spread quickly, in particular New York City, Chicago, and San Francisco.
Federal officials warn it’s still too soon to make pronouncements about the country turning a corner. Still the slowdown in some parts of the U.S. – coupled with data about how those at highest risk are protecting themselves and getting vaccinated – are promising signs.
“Our numbers are still increasing, [but] the rate of rise is lower,” Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention, told reporters on Friday. “We’re really hopeful that many of our harm reduction messages and our vaccines are getting out there and working.”
Reported case numbers have been trending down since mid August, based on an NPR analysis of data the CDC released Wednesday. Overall, there’s been around a 25% drop in the 7-day average of new cases over the past two weeks.
However, health officials caution that lags in data reporting can offer an incomplete picture of the outbreak in recent weeks, making it hard to know if cases have truly peaked.
The decline in parts of the U.S. mirrors what’s already being seen in some European countries, where the virus was detected a few weeks earlier. In both the U.K. and Germany, daily case counts have steadily dropped since late July. In several other countries, including the Netherlands and Italy, the number of new cases have plateaued.
Cases slow down in big cities
In New York City – one of the epicenters of the outbreak – the number of new people being infected has dropped 40% over the past month. San Francisco health officials are also seeing a decline in the rate of new cases.
“I’m cautiously optimistic,” says Dr. Susan Philip, health officer for the city and county of San Francisco. “We know, though, it’s going to take a lot of work and effort to sustain that downward curve and to make sure that cases continue to go down.”
The picture is also improving in other cities like Los Angeles, Houston and Chicago where local health leaders say there are indications that infections are leveling off.
Key metrics – such as the average number of cases and the time it takes for cases to double – have decreased over the past couple of weeks, says Janna Kerins, medical director at the Chicago Department of Public Health. “I’m not sure we’re ready to say this outbreak is truly ending,” Kerins says, “But all of those things are encouraging.”
The changes also track with modeling released this week that suggests the national outbreak is on the decline.
“We are seeing signs of a substantial slowdown and the forecasts suggest that this is going to go in the right direction,” at least over the next four weeks, says Gerardo Chowell-Puente, professor of epidemiology and biostatistics at the Georgia State University, who’s modeling the monkeypox outbreak
Changes in behavior drive the decline
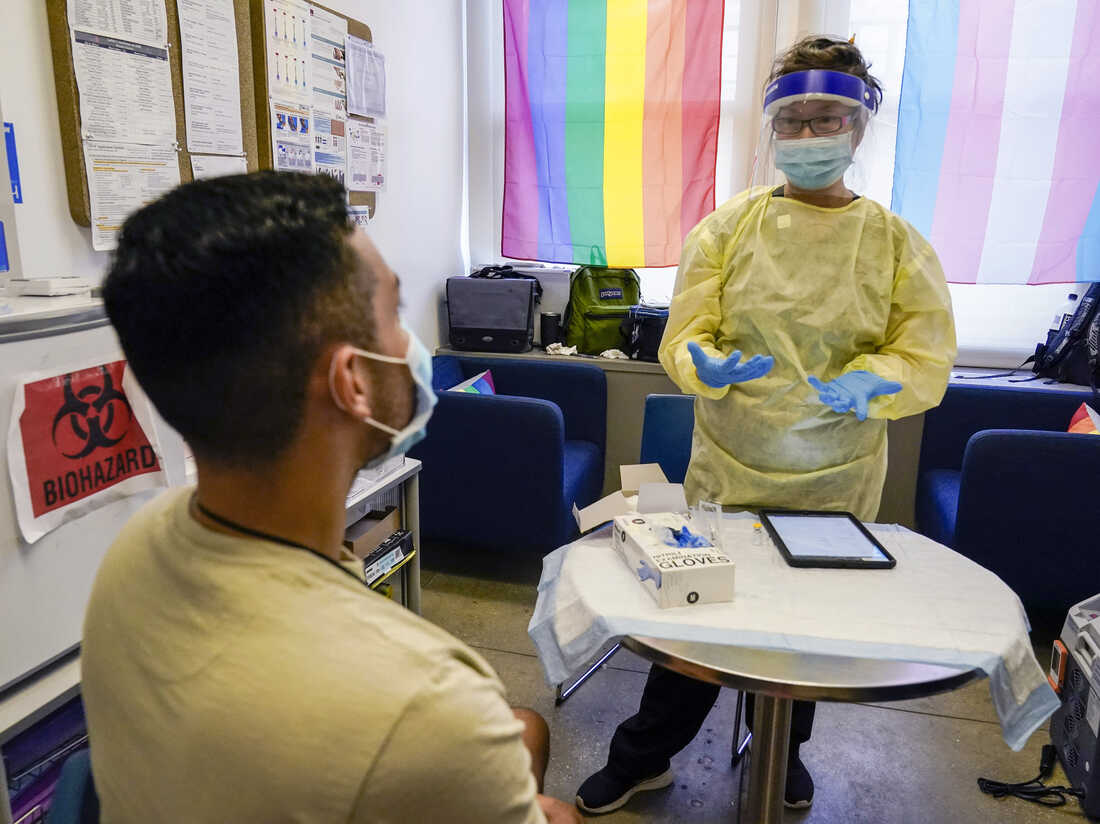
Given the size and diversity of the U.S., there’s still considerable uncertainty on how the outbreak will play out in different parts of the country, but infectious disease experts largely attribute the slowdown to efforts to change behavior among gay, bisexual and other men who have sex with men – a group that accounts for the vast majority of cases.
“Most of us in public health who work on this disease are quite confident that the majority of the reduction is due to change in behavior,” says Dr. Jay Varma, director of the Cornell Center for Pandemic Prevention and Response at Weill Cornell Medicine.
More than 94% of monkeypox cases in the U.S. are associated with sexual activity. And on Friday, CDC officials highlighted new data showing that gay and queer communities are modifying their sexual behaviors in response to messaging around monkeypox.
In one online survey, about 50% of respondents said they had reduced “their number of sexual partners, one-time sexual encounters [or] use of dating apps because of the monkeypox outbreak.” An accompanying modeling study released by the CDC showed that a “40% reduction in one-time sexual partnership might delay the spread of monkeypox and reduce the percentage of people infected” by up to about 30%.
“What this means is that the LGBTQIA+ people are doing things that are actually reducing their risk, and it’s working,” said Dr. Demetre Daskalakis, White House monkeypox response deputy coordinator, at a press briefing Friday.
It’s not entirely surprising that the virus appears to be slowing down in the U.S. as it has in Europe, says Dr. Jeffrey Klausner, a professor of medicine and infectious diseases, population and public health sciences at the Keck School of Medicine at the University of Southern California.
“Most of the cities will see a decline in cases – that decline may not be as fast or as steep as the ascent,” says Klausner.
Klausner notes that monkeypox has stayed mostly within certain relatively small sexual networks – that makes it harder for the virus to maintain momentum as vaccination increases, people build up immunity from infection and those at highest risk change their behavior.
“People who raised concerns about the spread of infection on college campuses and daycares and other kinds of settings where there’s close personal contact, at this point, that hasn’t occurred,” he says.
Uncertainty remains
But other experts are not as sanguine about the trajectory of the outbreak – at least not yet.
“It’s great to see some declines,” says Anne Rimoin, an epidemiologist at UCLA who has studied monkeypox for years. “But if the downward trend is due to changes in behavior and vaccinations, it’s not clear how long behavioral changes can be sustained, and how well the vaccinations actually work to prevent infections.”
Health officials are urging members of affected communities to keep taking precautions to slow the spread of monkeypox.
“Let me be clear,” Daskalakis said Friday. “The advice about how to reduce risk for monkeypox exposure is for now, not forever, and is an important part of our public health and community response as we urgently surge vaccinations to control this outbreak.”
Still, there isn’t robust real world data on how well the monkeypox vaccine – approved by the Food and Drug Administration in 2019 – protects against infection and transmission. Further complicating the picture is that a shortage of vaccine has led the Biden administration to pursue a new strategy of offering the shots intradermally in order to stretch the supply.
“The laboratory data that we have on the vaccine suggests that it’s going to be very effective in humans,” says Varma. “But what we know in medicine is that until we see what happens in the real world, we never know for sure.”
NPR’s Michaeleen Doucleff contributed to this report.
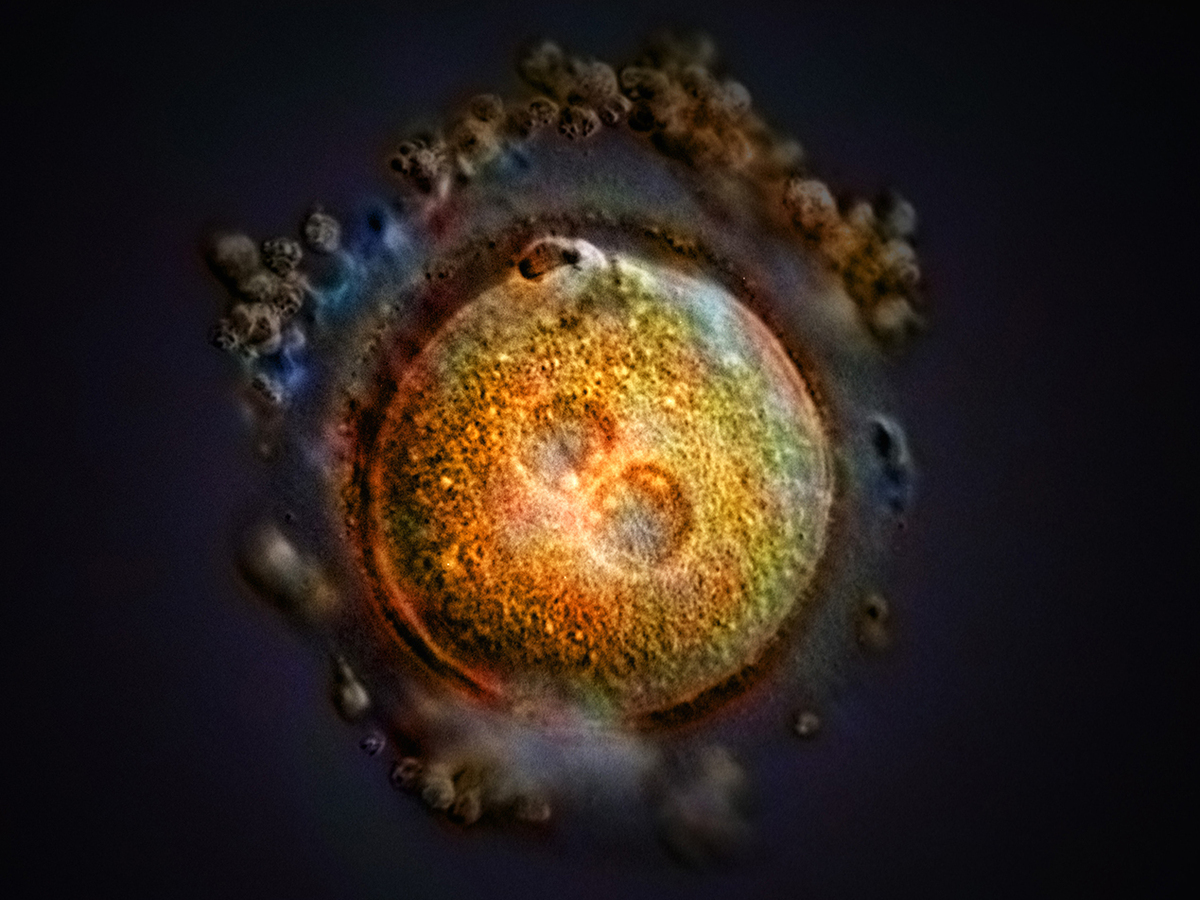
This computer-generated image shows the formation of a zygote after fertilization. Some Republican-led states, including Arkansas, Kentucky, Missouri, and Oklahoma, have passed laws declaring that life begins at fertilization, a contention that opens the door to a host of pregnancy-related litigation.
This computer-generated image shows the formation of a zygote after fertilization. Some Republican-led states, including Arkansas, Kentucky, Missouri, and Oklahoma, have passed laws declaring that life begins at fertilization, a contention that opens the door to a host of pregnancy-related litigation.
As life-preserving medical technology advanced in the second half of the 20th century, doctors and families were faced with a thorny decision, one with weighty legal and moral implications: How should we define when life ends? Cardiopulmonary bypass machines could keep the blood pumping and ventilators could maintain breathing long after a patient’s natural ability to perform those vital functions had ceased.
After decades of deliberations involving physicians, bioethicists, attorneys, and theologians, a U.S. presidential commission in 1981 settled on a scientifically derived dividing line between life and death that has endured, more or less, ever since: A person was considered dead when the entire brain — including the brainstem, its most primitive portion — was no longer functioning, even if other vital functions could be maintained indefinitely through artificial life support.
In the decades since, the committee’s criteria have served as a foundation for laws in most states adopting brain death as a standard for legal death.
Now, with the overturning of Roe v. Wade and dozens of states rushing to impose abortion restrictions, American society is engaged in a chaotic race to define the other pole of human existence: When exactly does human life begin? At conception, the hint of a heartbeat, a first breath, the ability to survive outside the womb with the help of the latest technology?
A legal and political maelstrom
That we’ve been able to devise and apply uniform clinical standards for when life ends, but not when it begins, is due largely to the legal and political maelstrom around abortion.
And in the two months since the U.S. Supreme Court issued its opinion in Dobbs v. Jackson Women’s Health Organization, eliminating a long-standing federal right to abortion, state legislators are eagerly bounding into that void, looking to codify into law assorted definitions of life that carry profound repercussions for abortion rights, birth control, and assisted reproduction, as well as civil and criminal law.
“The court said that when life begins is up to whoever is running your state — whether they are wrong or not, or you agree with them or not,” said Mary Ziegler, a law professor at the University of California-Davis who has written several books on the history of abortion.
Unlike the debate over death, which delved into exquisite medical and scientific detail, the legislative scramble to determine when life’s building blocks reach a threshold that warrants government protection as human life has generally ignored the input of mainstream medical professionals.
Instead, red states across much of the South and portions of the Midwest are adopting language drafted by elected officials that is informed by conservative Christian doctrine, often with little scientific underpinning.
A handful of Republican-led states, including Arkansas, Kentucky, Missouri, and Oklahoma, have passed laws declaring that life begins at fertilization, a contention that opens the door to a host of pregnancy-related litigation. This includes wrongful death lawsuits brought on behalf of the estate of an embryo by disgruntled ex-partners against physicians and women who end a pregnancy or even miscarry. (One such lawsuit is underway in Arizona. Another reached the Alabama Supreme Court.)
In Kentucky, the law outlawing abortion uses morally explosive terms to define pregnancy as “the human female reproductive condition of having a living unborn human being within her body throughout the entire embryonic and fetal stages of the unborn child from fertilization to full gestation and childbirth.”
Several other states, including Georgia, have adopted measures equating life with the point at which an embryo’s nascent cardiac activity can be detected by an ultrasound, at around six weeks of gestation. Many such laws mischaracterize the flickering electrical impulses detectible at that stage as a heartbeat, including in Georgia, whose Department of Revenue recently announced that “any unborn child with a detectable human heartbeat” can be claimed as a dependent.
Defining the role of government in life and death
The Supreme Court’s 1973 decision in Roe v. Wade that established a constitutional right to abortion did not define a moment when life begins. The opinion, written by Justice Harry Blackmun, observed that the Constitution does not provide a definition of “person,” though it extends protections to those born or naturalized in the U.S. The court majority made note of the many disparate views among religions and scientists on when life begins, and concluded it was not up to the states to adopt one theory of life.
Instead, Roecreated a framework intended to balance a pregnant woman’s right to make decisions about her body with a public interest in protecting potential human life. That decision and a key ruling that followed generally recognized a woman’s right to abortion up to the point medical professionals judge a fetus viable to survive outside the uterus, at about 24 weeks of gestation.
In decisively overturning Roe in June, the Supreme Court’s conservative majority drew on legal arguments that have shaped another contentious end-of-life issue. The legal standard employed in Dobbs — that there is no right to abortion in the federal Constitution and that states can decide on their own — is the same rationale used in 1997 when the Supreme Court said terminally ill people did not have a constitutional right to medically assisted death. That decision, Washington v. Glucksberg, is mentioned 15 times in the majority opinion for Dobbs and a concurrence by Justice Clarence Thomas.
Often, the same groups that have led the fight to outlaw abortion have also challenged medical aid-in-dying laws. Even after Dobbs, so-called right-to-die laws remain far less common than those codifying state abortion rights. Ten states allow physicians to prescribe lethal doses of medicine for terminally ill patients. Doctors are still prohibited from administering the drugs.
James Bopp, general counsel for the National Right to Life Committee who has been central to the efforts to outlaw abortion, said that both abortion and medically assisted death, which he refers to as physician-assisted suicide, endanger society.
“Every individual human life has inherent value and is sacred,” said Bopp. “The government has the duty to protect that life.”
Both issues raise profound societal questions: Can the government keep a patient on life support against his wishes, or force a woman to give birth? Can states bar their own residents from going to other states to end a pregnancy, or prohibit out-of-state patients from coming in to seek medically assisted death? And who gets to decide, particularly if the answer imposes a singular religious viewpoint?
A philosophical quandary
Just as there are legal implications that flow from determining a person’s death, from organ donation to inheritance, the implied rights held by a legally recognized zygote are potentially vast. Will death certificates be issued for every lost pregnancy? Will miscarriages be investigated? When will Social Security numbers be issued? How will census counts be tallied and congressional districts drawn?
Medical professionals and bioethicists caution that both the beginning and end of life are complicated biological processes that are not defined by a single identifiable moment — and are ill suited to the political arena.
“Unfortunately, biological occurrences are not events, they are processes,” said David Magnus, director of the Stanford Center for Biomedical Ethics.
Moreover, asking doctors “What is life?” or “What is death?” may miss the point, said Magnus: “Medicine can answer the question ‘When does a biological organism cease to exist?’ But they can’t answer the question ‘When does a person begin or end?’ because those are metaphysical issues.”
Ben Sarbey, a doctoral candidate in Duke University’s department of philosophy who studies medical ethics, echoed that perspective, recounting the Paradox of the Heap, a thought experiment that involves placing grains of sand one on top of the next. The philosophical quandary is this: At what point do those grains of sand become something more — a heap?
“We’re going to have a rough time placing a dividing line that this counts as a person and this does not count as a person,” he said. “Many things count as life — a sperm counts as life, a person in a persistent vegetative state counts as life — but does that constitute a person that we should be protecting?”
Even as debate over the court’s abortion decision percolates, the 1981 federal statute that grew out of the presidential committee’s findings, the Uniform Determination of Death Act, is also under review. This year, the Uniform Law Commission, a nonpartisan group of legal experts that drafts laws intended for adoption in multiple states, has taken up the work to revisit the definition of death.
The group will consider sharpening the medical standards for brain death in light of advances in the understanding of brain function. And they will look to address lingering questions raised in recent years as families and religious groups have waged heated legal battles over terminating artificial life support for patients with no brain wave activity.
Bopp, with the National Right to Life Committee, is among those serving on advisory panels for the effort, along with an array of doctors, philosophers, and medical ethicists. The concept of “personhood” that infuses the anti-abortion movement’s broader push for fetal rights is expected to be an underlying topic, albeit in mirror image: When does a life form cease being a person?
Magnus, who is also serving on an advisory panel, has no doubt the commission will reach a consensus, a sober resolution rooted in science. What’s less clear, he said, is whether in today’s political environment that updated definition will hold the same sway, an enduring legal standard embraced across states.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. It is an editorially independent operating program of KFF (Kaiser Family Foundation).
It has been estimated that over 54.4 million people in the United States have an autoimmune disease.1 Some of the major ones would be rheumatoid arthritis (RA), multiple sclerosis and inflammatory bowel diseases like Crohn’s and ulcerative colitis.
Since I have a massive clinical experience with RA I am going to use it as an example of how all autoimmune diseases can be treated. Why? Because they all have similar origins which are related to an antigen sneaking into your body and your immune system confusing it with one of your tissues that tags your tissue as a foreign invader. The antigen that gets into your system determines which of your body’s tissues will be impacted.
From the late 1980s and for the following 10 years I treated over 3,000 patients with rheumatic illnesses, including systemic lupus erythematosus (SLE), scleroderma, polymyositis and dermatomyositis. RA has a devastating prognosis in many patients.
Rheumatoid arthritis affects about 1% of our population and at least 1.4 million Americans have definite or classical rheumatoid arthritis, although it’s probably closer to 2 million.2 This number has increased in recent years, as in 2014 only about one half of a percent of the population suffered from RA.3
Since around 7 million Americans have some form of inflammatory rheumatic disease,4 this means you likely know someone with it. It is a much more devastating illness than previously appreciated. However, most patients with rheumatoid arthritis also have a progressive disability. This is important as the suggestions I am going to include should help improve all autoimmune diseases.
Testimonial From One of My Patients
I ran into a former patient, Sarah Allen, after giving a presentation in Orlando several years ago, where she happened to be in attendance. After talking to her, I decided we needed to share her important story as it would provide hope for so many who struggle with this disease. She first came to see me in August of 2003. Even though she was only 28 years old at the time, she’d been experiencing symptoms of RA for about three or four years. Sarah explains:
“I thought I was very healthy. I was young. I was a competitive triathlete. I believed I had a pretty good diet. So, I didn’t really understand why I was experiencing so much pain in my fingers and in my feet.
I had migrating pain, and a lot of tendonitis issues all throughout my body. It took the Western doctors a long time to diagnose me. It took about three years going to different doctors before they knew what was wrong. It didn’t show in my blood; I didn’t have the RA factor, and my C-reactive protein (CRP) levels were normal. But it showed up on an X-ray.”
Hallmark Signs of RA
One of the hallmark symptoms of rheumatoid arthritis is pain in your hands and/or feet. It tends to affect the proximal joints more so than the distal ones, i.e. the joints closest to your palm, for example, opposed to the joints further out in the fingers.
So, if you have pain there, especially if it’s symmetrical (affecting the same joints on both hands or feet), then almost by definition you have rheumatoid arthritis or an RA variant. It really doesn’t matter what the blood work shows.
RA is far less common than osteoarthritis, or degenerative joint disease, which is not as crippling and is a very different animal and should not be confused with it. It’s actually relatively easy to treat degenerative arthritis if you understand the components of a healthy lifestyle.
Rheumatoid arthritis is a far more complex disease. It’s an autoimmune disease; your body is destroying itself, and it can be terminal — some people have even been known to commit suicide from the crippling pain.
It’s quite notable that only a small percentage of people with the disease have a spontaneous, sustained remission without the help of medication.5 Some disability occurs in 50 to 70% of people within five years after onset of the disease, and half will stop working within 10 years.6
RA Is Typically Treated With Toxic Drugs
Traditional care also doesn’t have a lot of good hope for RA sufferers. All they do is ameliorate or treat the symptoms — typically using highly toxic drugs, including prednisone, methotrexate, and drugs that interfere with tumor necrosis factor, like Enbrel.
This is why I’m so passionate about spreading this information because as Sarah can attest, there’s an alternative, and this drug-free strategy really works. You don’t have to suffer needlessly in a conventional treatment model.
Once diagnosed, Sarah went to a well-known rheumatologist in Milwaukee who told her she needed to stop running or risk becoming permanently disabled. He prescribed a low-dose of methotrexate, which is actually an anticancer drug.
While it can be effective, the complications and the side effects are atrocious. Sarah had to check her liver status every month, and even though she was only on a low dosage for about three months, she started losing some of her hair. A rheumatology researcher at the Mayo Clinic whom she went to see told her to keep taking the drug, but expect it to shave 15 to 20 years off her life.
“I was really afraid of what that drug was going to do to my body,” Sarah says. “The physical therapist who recommended I get tested for RA said there was a lot I can do naturally. So I read a lot of books about rheumatoid arthritis and different alternative treatments.
I read there’s a possibility of it being connected with an infection, and that a low dose of antibiotics was being prescribed. I then came across your name in a book. I looked you up, found you in Chicago, and made an appointment.”
Dr. Brown’s Protocol
The book she’s referring to is “The Road Back: Rheumatoid Arthritis — Its Cause and Its Treatment,” written by Dr. Thomas McPherson Brown and Henry Scammell. Brown was a well-respected board-certified rheumatologist (he passed away in 1989), but he, like me, was a rebel.
He didn’t agree with the use of prednisone, which was the standard of care for RA in the ’40s and ’50s. He believed RA was an infection caused by mycoplasmas, so he used the antibiotic tetracycline instead.
Eventually, he modified his treatment to more potent discriminating forms of tetracycline, such as minocycline. Brown ultimately helped bring over 10,000 patients into remission. I first saw his work in a “20/20” special done shortly before he died in 1989, and it really inspired me. I decided to study his work, began using his protocol on RA patients in my practice, and was really impressed with the results. Eventually I modified the protocol to the point where I abandoned antibiotics altogether.
There are a number of physicians that still use his protocol,7 but it would be uncommon to find ones that will be using all of what I consider the vital elements to successfully reversing RA that I list below. If you see one of these physicians, I would encourage you do integrate every one of the elements below.
So, listed below are the steps that I believe are absolutely crucial to integrate in the reversal of not only RA but all autoimmune diseases.
Optimize Your Vitamin D Levels Without Pills
Since RA is an autoimmune disease it is vital to optimize your vitamin D level. That is the most basic and least expensive strategy that one can easily implement. The early part of the 21st century brought enormous attention to the importance and value of vitamin D, particularly in the treatment of autoimmune diseases like RA.
From my perspective, it is now virtually criminal negligent malpractice to treat a person with RA and not aggressively monitor their vitamin D levels to confirm that they are in a therapeutic range of 50 to 70 ng/ml.
It is also vitally important to understand that your body was designed to get all the vitamin D it needs from the sun. I have not swallowed vitamin D in two decades, yet am able to routinely get my levels up to 90 ng/ml. So the KEY is to get about one hour of sun exposure a day around solar noon, which is 1 p.m. if you are in Daylight Saving Time, with minimal clothing on. Ideally you can walk during this time so you get your movement in.
The reason why this is so important is that getting vitamin D from the sun also provides many other benefits than vitamin D optimization, such as:
It increases subcellular mitochondrial melatonin which will radically lower oxidative stress where you need it most: In the electron transport chain of the mitochondria. Not only is melatonin a powerful antioxidant, but it causes your body to produce glutathione which is essential for controlling oxidative stress.
Males will be pleased to know that a 2021 study8 showed that sun exposure for around 30 minutes near solar noon will increase testosterone levels.
It will increase structured water in your body, which greatly facilitates red blood cell transport through your capillaries.
It will increase nitric oxide to help optimize your blood pressure.
It will help convert vitamin A (retinol) to retinoids which is required for optimal immune functioning.
Many are likely concerned about sunburn and skin cancer when considering solar skin exposure. The key is to understand that the largest factor contributing to this is excess omega-6 fat that contains linoleic acid (LA). Seed oils and processed foods need to be avoided as reviewed in another section on this page.
They are loaded with LA, which is the main reason why skin cancers like basal cell and squamous cell carcinoma occur. If you have a low LA intake you will likely not burn or get skin cancers.
Sadly, most are unable to get enough UVB from the sun in late fall to early spring unless you live below the 20th latitude. Ideally it would be far better to optimize your vitamin D by safe exposure of your skin to UVB. Even better would be to make sure that you get concurrent near infrared (IR) exposure at the same time as this will increase melatonin to suppress any free radical damage from the UVB.
Make sure to take 500 mg to 1000 mg of magnesium and 150 mcg of vitamin K2, (not K1) which are important cofactors for optimizing vitamin D function. And, remember the only way you know what your vitamin D level is, is to test it. Most people I know are shocked how low their level is when they finally get around to testing it.
Ultra-Low Seed Oil Diet
While considered an essential fat, when consumed in excessive amounts — which over 99% of people do — LA (an omega-6 polyunsaturated fat or PUFA) acts as a metabolic poison.
Most clinicians who value nutritional interventions to optimize health understand that vegetable oils, which are loaded with omega-6 PUFA, are something to be avoided. What most fail to appreciate is that even if you eliminate the vegetable oils and avoid them like the plague, you may still be missing the mark.
Chances are you’re still getting too much of this dangerous fat from supposedly healthy food sources such as olive oil and chicken (which are fed LA-rich grains). Another common mistake is to simply increase the amount of omega-3 that you eat. Many are now aware that the omega-3 to omega-6 ratio is very important, and should be about equal, but simply increasing omega-3 can be a dangerous strategy.
Over the last century, thanks to fatally flawed research suggesting saturated animal fat caused heart disease, the LA in the human diet has dramatically increased, from about 2 to 3 grams a day 150 years ago, to 30 or 40 grams a day today. LA used to make up 1% to 3% of the energy in the human diet and now it makes up 15% to 20%.
It is my belief that this radical change has had the most catastrophic impact on human health in the history of the human race. This dietary change has undoubtedly killed millions, probably hundreds of millions, prematurely and still continues to do so because people, and more importantly, nearly all physicians simply don’t understand this.
At a molecular level, excess LA consumption damages your metabolism and impedes your body’s ability to generate energy in your mitochondria. It is also likely the primary factor for the increases in obesity, cancer, heart disease, diabetes and dementia that have exploded the past century.
There’s also compelling evidence showing eliminating seed oils from your diet will dramatically reduce your risk of sunburn and skin cancer. Susceptibility to UV radiation damage is controlled by how much LA is in your diet. It’s like a dial that can control how fast it happens, and how fast you get skin cancer.
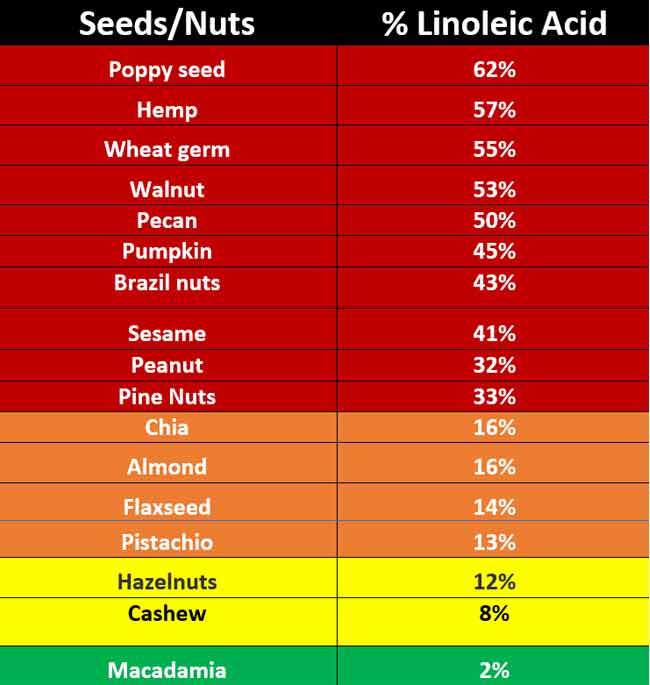
You can use the tables below to help you get a handle on the amount of LA in your diet. You can also use Cronometer.com to enter the foods you eat to identify just how much LA you are eating.
Time Restricted Eating (TRE) and Circadian Rhythm Optimization
In July of 2022 we learned that fewer than 1 in 14 adults in the U.S. have optimal cardiometabolic health.9 This means they lack the ability to seamlessly shift between burning fat and carbs as their primary fuel source and as a result have impaired immune function.
It would seem profoundly obvious that having an immune system would not be good if you had an autoimmune disease. Fortunately, there is a simple inexpensive intervention that can help most everyone with this issue and it is called TRE.
Research by Satchidananda Panda, Ph.D., suggests 90% of people eat for more than 12 hours a day, and over time this habit will wreak havoc on your metabolism and limit your ability to metabolize fat as a primary fuel. When you eat throughout the day and never skip a meal your body adapts to burning sugar as your primary fuel, resulting in the downregulation of enzymes that utilize and burn stored fat.10,11
As a result, you become progressively more insulin resistant and start gaining weight. Efforts to lose weight also become ineffective for this very reason, since to lose body fat, your body must first be able to actually burn fat. Many biological repair and rejuvenation processes also take place while you’re fasting, and this is another reason why all-day grazing triggers diseases while fasting prevents them.
Time-restricted eating is just what it sounds like. It’s a form of intermittent fasting where you eat all of your meals for the day within a restricted window of time, ranging from six to eight hours. That means you’re avoiding food (fasting) for 16 to 18 consecutive hours. Eating within a six to eight-hour window is likely close to metabolically ideal for most. Eighteen-hour TRE windows work better for overweight people and 16-hour TRE windows are used for normal weight individuals.
The key is to make sure you don’t start your TRE window too late in the day. Ideally the last food you eat should be at least three to five hours before you go to sleep. The last thing you want to do is eat right before bed as that will impair your health.
Contrary to longer fasts and calorie restriction, TRE is a strategy that can work for just about anyone. Remember, you’re not actually limiting or counting calories. Weakness and lethargy, which are signs of undernourishment, simply don’t occur. It’s a practice that should make you feel fantastic and actually reduce your hunger over time. Wouldn’t it be great to not be controlled by hunger and sweets anymore?
Circadian Optimization
Satchin Panda is one of the leading researches in circadian rhythm and I interviewed him about his book, “Circadian Code: Lose Weight, Supercharge Your Energy, and Transform Your Health From Morning to Midnight.” He has many great tips in his book on how to optimize your circadian cycle. This is important as it supports a healthy immune system.
If you think about the times you got sick in the past my guess is that many of those times were related to altered or impaired sleeping schedules. This is a classic illustration of how important this strategy is. Here are some tips to optimize your circadian rhythm:
• Be sure your sleep timing is close to the natural day and night cycles. The closer you are to the equator or vernal or autumnal equinox the easier that is, as the day and night time is evenly divided between them at 12 hours each. The further you move away the worse the change is all the way to the polar extremes of 24 hours of night in the winter to 24 hours of light in the summer.
• Ideally you should not have any blue light after sundown. Unfortunately, the invention of the electric light bulbs has trashed our circadian cycles. The ideal light would be a candle as it has the right wavelengths and intensity.
Alternatively, a 3-watt non-flicker red LED light12 is acceptable and will not likely impair your circadian cycle. You should also make certain that there is no light in your bedroom while you are sleeping; use a sleep mask, if necessary, to get into complete darkness.
• EMF exposure, especially in the night, can disrupt your cycle and your health. It is ideal if you turn off both your Wi-Fi and phone at night, or at least keep it in airplane mode. The last thing you need at night is exposure to these fields, as it will impair your health.
Low-Dose Naltrexone (LDN)
One new addition to the protocol is low-dose naltrexone (LDN), which I would encourage anyone with RA to try. It is inexpensive and nontoxic and I have a number of physician reports documenting incredible efficacy in getting people off of all their dangerous arthritis meds. Although this is a drug, and strictly speaking not a natural therapy, it has provided important relief and is FAR safer than the toxic drugs that are typically used by nearly all rheumatologists.
Naltrexone is similar to Naloxone (Narcan), which is a narcotic antagonist to save people’s lives in opioid overdoses. In low or even microdoses it is one of the few pharmaceutical drugs I wholeheartedly endorse and it is remarkably safe.
Naltrexone blocks the opioid receptor only briefly, and by a different mechanism. When used in low dosages as LDN, the chief benefit is actually in the rebound effect, after the opioid receptor has been briefly blocked. Naltrexone is one of the few interventions that actually enables your own body and immune system to be able to function better and restore function.
Naltrexone is a drug and requires a prescription from a doctor willing to work with you. Dosing guidelines can be found at ldnresearchtrust.org/2022_LDN_Guides. I also did an interview with Linda Elsegood, a Briton who founded the LDN Research Trust in 2004, and Dr. Sarah Zielsdorf, who has a medical practice in the Chicago about the book they wrote.13
Carnivore Diet
I would strongly recommend implementing every one of the above strategies. If you are still not getting the improvement you need and deserve, then it may be time to consider removing all vegetables from your diet.
In the video above, Mikhaila Peterson, the daughter of best-selling author Jordan Peterson, discusses how she resolved her juvenile rheumatoid arthritis (JRA), which is relatively uncommon, but notoriously challenging to improve. Her results are nothing less than spectacular and certainly provide enough anecdotal confirmation to give this unconventional but safe approach a try.
For the scientific justification and help in implementing a carnivore diet, one of the best resources out there is Paul Saladino, who wrote the book, “The Carnivore Code: Unlocking the Secrets to Optimal Health by Returning to Our Ancestral Diet,” and also has a podcast on YouTube called “CarnivoreMD.”
The reason why avoiding plants might provide relief with autoimmune diseases is that they are loaded with self-defense chemicals and antinutrients such as the following:
Nightshades — The solanaceae family of flowering plants includes a number of species that are outright poisonous. But the nightshade family also includes tomatoes, potatoes, peppers, eggplant and goji berries, which are well-known to promote inflammation and joint pain in some people.
Phytic acid — A natural substance found in plant seeds (including grains and legumes), this compound is known as an “antinutrient” for its ability to bind to minerals. Phytic acid impairs the absorption of iron, zinc, calcium and other minerals and can promote mineral deficiencies.
Oxalates — Compounds found in dark leafy greens, such as spinach, kale and other “superfoods.” Most people can break down oxalates in the gut. For others, however, these compounds turn into sharp crystals and can lead to chronic pain, inflammation, oxidative stress, kidney stones and autoimmune disease.
Lectins — These plant compounds can promote leaky gut, alter the microbiome, stimulate the immune system and trigger inflammation. The highest levels are found in whole grains, legumes and dairy.
Salicylates — These are naturally-occurring pesticides that plants use to protect against insects, fungus and bacterial infection. In humans, they can cause a wide range of symptoms from tinnitus to ulcers. High concentrations are found in avocados, berries, grapes, almonds, honey, dried fruits and many spices.
FODMAPs — Though not technically a defense mechanism of plants, these compounds are a collection of short-chain carbohydrates that are not properly absorbed in the gut. FODMAPs can cause severe digestive distress for some people. High-FODMAP foods include a wide range of fruits, vegetables, cereal grains, condiments, drinks and dairy foods.
Saponins — Antifeedant compounds that protect many plants from predation by insects, microbes and fungi, saponins have soapy, foaming characteristics. They promote leaky gut and can cause bloating, gas, nausea and diarrhea. Legumes (soy, beans, peas and lentils) as well as quinoa are rich in saponins.
Goitrogens — These compounds can reduce iodine uptake in the thyroid gland and slow the production of thyroid hormones. The result can be an enlarged thyroid (goiter) and a host of metabolic disturbances. The most common plant goitrogens are compounds known as glucosinolates found in broccoli, cauliflower, Brussels sprouts, cabbage, kale, arugula, radishes, turnips, collard greens, bok choy and other similar vegetables.
Phytoestrogens — These naturally-occurring plant chemicals have a molecular structure quite similar to estrogen. Used as a natural defense against herbivores, they can disrupt animal fertility. In humans, phytoestrogens can cause hormonal dysfunction and may promote cancer. These compounds are most common in soybeans, flax and sesame seeds.
Prolamins and glutelins — Consisting of a wide range of proteins used by plants to store energy in seeds and found primarily in grains and rice, this group of compounds harbors the primary environmental factors in causing Celiac disease.
Early Emotional Traumas Are Pervasive in Autoimmune Diseases
With the vast majority of the patients I treated, some type of emotional trauma occurred early in their life, before the age that their conscious mind was formed, which is typically around the age 5 or 6. However, a trauma can occur at any age, and has a profoundly negative impact.
If that specific emotional insult is not addressed with an effective treatment modality, then the underlying emotional trigger will continue to fester, allowing the destructive process to proceed, which can predispose you to severe autoimmune diseases like RA later in life.
In some cases, RA appears to be caused by an infection, and it is my experience that this infection is usually acquired when you have a stressful event that causes a disruption in your bioelectrical circuits, which then impairs your immune system.
This early emotional trauma predisposes you to developing the initial infection, and also contributes to your relative inability to effectively defeat the infection. Therefore, it’s very important to have an effective tool to address these underlying emotional traumas. In my practice, the most common form of treatment is called the Emotional Freedom Technique (EFT).
Although EFT is something that you can learn to do yourself in the comfort of your own home, it is important to consult a well-trained professional to obtain the skills necessary to promote proper healing using this amazing tool. There are, of course, many other strategies other than EFT that can address these; EFT is just the one that I have the most experience with.
This article was previously published June 12, 2019, and has been updated with new information.
According to polls, the No. 1 reason people choose organic food is to avoid pesticide exposure.1 Not only do these chemicals threaten the environment, but they also pose a very clear and direct risk to human health.
Glyphosate, the active ingredient in Monsanto’s Roundup herbicide — identified as a probable human carcinogen by the International Agency for Research on Cancer (IARC)2,3 in 2015 — is the most heavily used agricultural chemical in history.4
A 2016 study5 published in Environmental Sciences Europe revealed use of glyphosate rose nearly fifteenfold between 1996 (when Roundup Ready crops were introduced) and 2014. Between 1974 and 2014, 1.8 million tons of glyphosate were applied to U.S. fields. The global total for that timeframe was 9.4 million tons.
Mounting evidence shows the weed killer is nowhere near as effective as it used to be, thanks to mounting resistance, and there are more than 13,000 pending lawsuits6 charging Monsanto’s (now Bayer’s7,8) herbicide Roundup caused the plaintiffs’ Non-Hodgkin lymphoma.
Despite that, a recent data analysis9 by the Midwest Center for Investigative Reporting shows usage hasn’t dropped off. On the contrary, glyphosate use has dramatically increased across the Midwest in recent years.
Glyphosate Use Shows No Signs of Decline in Midwest
Writing for the Midwest Center for Investigative Reporting, Christopher Walljasper and Ramiro Ferrando point out that “Nationwide, the use of glyphosate on crops increased from 13.9 million pounds in 1992 to 287 million pounds in 2016, according to estimates by the U.S. Geological Survey.”10
In 2016, Midwest farmers used an estimated 188.7 million pounds of glyphosate, a fortyfold increase from 1992, and the Midwest accounts for 65% of the total glyphosate usage in the U.S. Some states have seen an even greater increase.
In Nebraska, Indiana, Illinois, Minnesota and Iowa, glyphosate usage was about 80 times greater in 2016 than in 1992, and 15 times higher than in 2000. According to an August 2022 glyphosate market report, the global glyphosate market is also predicted to continue growing, from $4.44 billion in 2020 to $5.24 billion by 2027.11
While this seems like a huge increase, actually it’s substantially lower than the $8.8 billion predicted only five months earlier, in March 2022. The decrease is due to what Reuters called “off the charts” shortages of the chemical.12
GMOs Have Been a Primary Driver of Toxic Weed Killer Use
Despite a slower rise in sales, one of the reasons for any increase is that genetically engineered corn and soybeans dominate this agricultural area, and glyphosate is routinely used on these crops as they are designed to survive direct application. Walljasper and Ferrando write:13
“Once thought of as a miracle product, overreliance on glyphosate has caused weeds to grow resistant to the chemical and led to diminished research and development for new weed management solutions, according to Bill Curran, president-elect of the Weed Science Society of America and emeritus professor of weed science at Penn State University.
‘We’re way overreliant on roundup,’ Curran said. ‘Nobody thought we were going to be dealing with the problems we are dealing with today’ … James Benham has been farming in Southeast Indiana for nearly 50 years. Benham said, as resistance grew, Roundup went from a cure-all to a crutch. ‘Sometimes if you timed it just right, you could get away with just one spraying. Now we’re spraying as often as three or four times a year,’ he said.
Benham said farmers continue to spend more on seed and chemicals but aren’t seeing more profit. ‘That puts the farmer in that much more of a crisis mode. Can’t do without it, can’t hardly live with it,’ he said. As glyphosate became less effective, farmers also turned to even more pesticides to try and grow successful crops each year.”
Be Very Careful How You Measure Your Glyphosate Levels
There are only a few companies that test not only for glyphosate but its breakdown product AMPA. I have had many tests for glyphosate from HRI Labs. It is my absolute most preferred lab to use for this toxin. They use state of the art mass spectroscopy and have incredibly accurate results.
In every HRI test I have done, both glyphosate levels were either undetectable or were trace. HRI is in the process of doing hair testing for glyphosate, which is a better test for long-term exposure. I was surprised when mine came back higher than trace as I eat only organic.
But the really important point of this section is to warn you that if you use a lab other than HRI, you need to be really careful. Just for grins, I sent a sample to a popular lab for glyphosate and was shocked when I received my results in the absolutely nonstandard cryptic units of micrograms/gram of creatinine.
What was even more surprising was that it was seriously higher than any test I had done at HRI. So, I dug deeper and called the owner of the lab and conference called in with the director of the HRI lab and we found out the problem. They are using a vastly inferior RIA test for glyphosate. The test is very accurate in water, but when testing for glyphosate in urine like they do, it comes back falsely high.
So, the bottom line is be careful out there. If you are using a lab other than HRI for testing for glyphosate, look at the units that your test results are reported in. It needs to be in parts per billion (ppb). If it is in micrograms/gram of creatinine, please realize that your results are seriously misleading. I have encouraged the owner of the lab to switch but, sadly, he refused. So, your best approach right now is to avoid using labs that don’t measure in ppb.
Will Billions in Legal Damages Taper Glyphosate Sales?
As noted by Walljasper and Ferrando, a number of lawsuits against Monsanto/Bayer have resulted in high damages, but while Bayer’s stock price dropped by more than 44% after its takeover of Monsanto in 2018,14 there wasn’t a noticeable slowdown in Roundup sales until mid-2022, when the COVID pandemic created supply-chain issues.15
Not surprisingly, since IARC linked glyphosate to an increased risk for Non-Hodgkin lymphoma in 2015,16,17 the number of cancer victims suing for damages has skyrocketed, and the link between glyphosate and Non-Hodgkin lymphoma has only grown stronger.
More recently, a meta-analysis18,19,20,21 of six epidemiological studies published between 2001 and 2018 found glyphosate increases the risk of Non-Hodgkin lymphoma by 41% in highly exposed subjects. Of the six studies included in this new analysis, five showed a positive correlation.
One of the studies, known as the Agricultural Health Study,22 published in 2018, found no effect. However, the researchers point out that results were watered down in that study due to the inclusion of people with very low exposure. It’s only when you look at high-exposure groups independently that a clear link between exposure and Non-Hodgkin lymphoma emerges. The following are three examples:
The first case against Monsanto to go to court resulted in 46-year-old Dewayne Johnson, who is terminally ill with Non-Hodgkin lymphoma, being awarded $289 million in damages. The judge reduced the total award to $78 million.23,24,25 and then again to just $20.5 million on an appeal by Monsanto/Bayer. The case is now closed.26
In the second case to be heard, the jury awarded 70-year-old plaintiff Edwin Hardeman $80 million in damages.27,28 Although Monsanto/Bayer appealed Hardeman’s award all the way to the U.S. Supreme Court, the court denied to hear the appeal in June 2022.29 In a summary of the case, AgriPulse noted that the ag company had settled more than 100,000 cases so far, with 30,000 still waiting.30
The third case, brought before the Alameda County Superior Court of California, involved a married couple, Alva and Alberta Pilliod, both of whom claimed they developed Non-Hodgkin lymphoma after regular, long-term use of Roundup.
As in the previous two court cases, the jury found Monsanto acted with negligence as they chose not to warn consumers about cancer risks, and the Pilliods were awarded $2.055 billion in combined damages.31,32,33
Monsanto/Bayer appealed in this case, too, and a judge reduced the verdict to $86.7 million, a number which stayed after the ag company lost in a District Court of Appeal in San Francisco in 2021.34 These three cases have all involved patients with Non-Hodgkin lymphoma, but glyphosate-based herbicides have also been linked to several other types of lymphatic cancers and blood cancers.35
As reported by Bloomberg,36 a class-action lawsuit filed against Monsanto February 13, 2019, specifically focuses on glyphosate’s effect on gut bacteria, which we now know play vital roles in human health and can influence everything from mood to chronic diseases of all kinds.
According to this lawsuit, Roundup’s label falsely assures consumers that the product works by targeting an enzyme not found in people or animals. Research has proven this false, as this enzyme does exist in human and some animal gut bacteria.37
As mentioned, as of August 2022, more than 100,000 individuals harmed by Roundup had settled with the company, to the tune of $11 billion, with tens of thousands more cases pending.38
The Many Ways in Which Glyphosate Harms Your Health
Were the full ramifications of glyphosate fully understood, there’s no doubt it would be banned. The question is, just how much evidence do we need? There’s already ample research showing glyphosate can harm health in a wide variety of ways. For example:
Research39 published in 2007 found that aerial spraying of glyphosate in combination with a surfactant solution resulted in DNA damage in those exposed.
Research40 published in 2015 found that glyphosate in combination with aluminum synergistically induced pineal gland pathology, which in turn was linked to gut dysbiosis and neurological diseases such as autism, depression, dementia, anxiety disorder and Parkinson’s disease. According to the authors:
“The pineal gland is highly susceptible to environmental toxicants. Two pervasive substances in modern industrialized nations are aluminum and glyphosate … In this paper, we show how these two toxicants work synergistically to induce neurological damage.
Glyphosate disrupts gut bacteria, leading to an overgrowth of Clostridium difficile. Its toxic product, p-cresol, is linked to autism in both human and mouse models. p-Cresol enhances uptake of aluminum via transferrin.
Anemia, a result of both aluminum disruption of heme and impaired heme synthesis by glyphosate, leads to hypoxia, which induces increased pineal gland transferrin synthesis. Premature birth is associated with hypoxic stress and with substantial increased risk to the subsequent development of autism, linking hypoxia to autism.
Glyphosate chelates aluminum, allowing ingested aluminum to bypass the gut barrier. This leads to anemia-induced hypoxia, promoting neurotoxicity and damaging the pineal gland.
Both glyphosate and aluminum disrupt cytochrome P450 enzymes, which are involved in melatonin metabolism. Furthermore, melatonin is derived from tryptophan, whose synthesis in plants and microbes is blocked by glyphosate.
We also demonstrate a plausible role for vitamin D3 dysbiosis in impaired gut function and impaired serotonin synthesis. This paper proposes that impaired sulfate supply to the brain mediates the damage induced by the synergistic action of aluminum and glyphosate on the pineal gland and related midbrain nuclei.”
Glyphosate also inhibits pituitary release of thyroid stimulating hormone, which can lead to hypothyroidism.41
Glyphosate mimics glycine (the “gly” in glyphosate stands for glycine), an amino acid your body uses to make proteins. By acting as a substitute for glycine in your body, glyphosate can cause damaged proteins to be produced. As noted in the 2017 paper,42 “Glyphosate Pathways to Modern Diseases VI: Prions, Amyloidoses and Autoimmune Neurological Diseases”:
“In this paper we explain how glyphosate, acting as a non-coding amino acid analogue of glycine, could erroneously be integrated with or incorporated into protein synthesis in place of glycine, producing a defective product that resists proteolysis. Whether produced by a microbe or present in a food source, such a peptide could lead to autoimmune disease through molecular mimicry.”
Glycine also plays a role in quenching inflammation, and is used up in the detoxification process. As a result of glyphosate toxicity, many of us may not have enough glycine for efficient detoxification.
Glyphosate chelates important minerals, including iron, cobalt and manganese. Manganese deficiency, in turn, impairs mitochondrial function and can lead to glutamate toxicity in the brain.43
By impairing serotonin transport and killing beneficial gut bacteria (glyphosate is in fact an antibiotic), glyphosate may also contribute to a wide range of mood disorders, including major depression.44
By interfering with the function of cytochrome P450 enzymes, glyphosate also interferes with the activation of vitamin D in the liver and the creation of both nitric oxide and cholesterol sulfate, the latter of which is needed for red blood cell integrity.45
According to research46 presented at a 2017 Children’s Environmental Health Network conference in Washington, D.C., women exposed to higher glyphosate levels during pregnancy had babies born earlier and with lower adjusted birth weights. What’s more, the chemical was detected in more than 90% of the mothers in the study.
A thorough review of published studies47 showing human and animal health effects has been compiled by Drs. Alex Vasquez and Eva Sirinathsinghji, and can be accessed on I-SIS.org, hyperlinked above. It contains 220-pages’ worth of research — more than enough to satisfy most critical thinkers.
Another illuminating and heavily referenced 80-page report48 is “Banishing Glyphosate,” written Eva Sirinathsinghji and the late Mae-Wan Ho, with cooperation from six other researchers, including Don Huber and Nancy Swanson.
(Huber has also written a 42-page report49 titled “Ag Chemicals and Crop Nutrient Interactions,” in which he explains how extensive use of glyphosate and the adoption of glyphosate-tolerant GE crops have resulted in essential micro- and macronutrient deficiencies in plants, and the increased need for micronutrient remediation in the soil.)
In the 2015 paper50 “The High Cost of Pesticides: Human and Animal Diseases,” Judy Hoy, an expert on Montana wildlife, along with Swanson and Stephanie Seneff, Ph.D., poured through data from the Centers for Disease Control and Prevention’s database, looking for correspondences between animal- and human disease, and correlations with pesticide usage.
Several of the plotted charts show animal- and human diseases rising in step with glyphosate usage on corn and soy crops. This includes conditions such as failure to thrive, congenital heart defects, enlarged right ventricle, liver cancer, and in newborns: lung problems, metabolic disorders and genitourinary disorders.
Testing Reveals Widespread Contamination of Food Supply
All of this evidence raises serious questions about the safety of glyphosate-contaminated foods. Testing has revealed more than 70% of Americans have detectable levels of glyphosate in their bodies,51 and food testing shows surprisingly widespread contamination of the food supply. For example:
A limited food testing program by the U.S. Food and Drug Administration in 2016 revealed virtually all foods tested were contaminated with Roundup.52
Test results53 published in August 2018 by the Environmental Working Group (EWG) showed 43 out of 45 food products made with conventionally grown oats tested positive for glyphosate, 31 of which had glyphosate levels higher than EWG scientists believe would be safe for children.
A second round of EWG testing54,55 revealed glyphosate is a staple contaminant in Cheerios breakfast cereals and Quaker oats products. All 28 samples contained glyphosate; 26 at levels suspected to be harmful to children’s health. Five of 16 organic oat foods also contained low amounts of glyphosate, even though glyphosate is prohibited in the U.S. organic standards.
Testing by the Health Research Institute Labs (HRI Labs), an independent laboratory that tests both micronutrients and toxins found in food, confirms reports of severe contamination, showing that people who eat oats on a regular basis have twice as much glyphosate in their system as people who don’t, and people who eat organic food on a regular basis have an 80% lower level of glyphosate than those who rarely eat organic.
Testing57 by Moms Across America found glyphosate in PediaSure Enteral Formula nutritional drink, which is given to infants and children via feeding tubes; 30% of the samples tested contained levels of glyphosate over 75 ppb — far higher levels than have been found to destroy gut bacteria in chickens (0.1 ppb).58
Testing by The Detox Project shows glyphosate contamination is rampant in organic plant-based protein supplements as well.59,60 When testing eight of the most popular pea protein brands sold on Amazon.com as of March 2019, one organic brand was found to contain as much or more glyphosate than conventional brands.
Two conventional (nonorganic) brands, Naked Pea and Anthony’s Pea Protein, had 39 ppb and 80 ppb respectively, while two separate batches of a top-selling organic brand, Orgain Organic Plant-Based Protein Powder, contained 83 ppb and 281 ppb. According to The Detox Project,61 zero to 9 parts per billion (ppb) of glyphosate is a nondetectable level of no concern; 10 to 79 ppb is trace amounts of slight concern; anything above 80 ppb is of high concern.
Why Such Widespread Contamination?
One of the reasons so many processed foods are contaminated with glyphosate has to do with the fact that most contain GMO ingredients. Roundup Ready GMO crops are designed to survive direct dousing of Roundup, which gets incorporated into every cell of the plant. Since the glyphosate cannot be washed off, and every part of the final grain is contaminated, it ends up in the final food product as well.
However, it has now become clear that the problem is not restricted to GMO ingredients. Farmers are also using glyphosate as a desiccant or drying agent to speed up harvesting and increase yield of non-GMO grains and legumes.62,63 This is why we find glyphosate even in non-GMO products.
It’s still unclear how the chemical is ending up in some organic products. Possible causes include drift from nearby conventional and/or GE crop fields, contamination during processing, and fraud (where a nonorganic crop is sold as organic).
While glyphosate is commonly used as a preharvest drying agent,64,65 it’s not a registered (i.e., approved) desiccant.66 Farmers who use glyphosate anyway, and douse their crops at the wrong time, can cause their crop to be heavily contaminated.
As explained in “Clarification of Preharvest Uses of Glyphosate,”67 if glyphosate is applied too early (while the grain has a moisture rate higher than 30%), the glyphosate is absorbed through the leaves and stems and translocates throughout the plant.
How Much Glyphosate Do You Have in Your Body?
Considering how pervasive glyphosate is in the U.S. food supply, chances are you and your children have been exposed. The only way to determine to what degree your diet is exposing you to this toxic contaminant is to get tested. HRI Labs has developed home test kits for both water and urine, available in my online store. I do not make a profit from the sale of these kits. I only provide them as a service of convenience.
If your glyphosate levels are high, you would be wise to address your diet and consider buying more organic foods. Studies68,69,70,71 have demonstrated organic foods significantly lower your exposure to toxic pesticides and lower your overall toxic burden.
The most recent of these studies72,73 was published in the journal Environmental Research, February 12, 2019, showing just how rapidly you can lower your pesticide load by switching to organic.
On average, pesticide and pesticide metabolite level for neonicotinoids, organophosphate pesticides, pyrethroid, 2,4-D and others (14 compounds in all, representing about 40 different pesticides) were reduced by more than 60%, on average, in just six days of eating an all-organic diet. As a group, organophosphate pesticides (such as glyphosate) were reduced the most, dropping by 70% overall.
Many studies74,75,76,77,78,79,80,81 also show organic foods contain higher amounts of valuable nutrients, so going organic makes for a more nutritious diet overall. You may also want to consider some form of detoxification protocol, and take steps to repair the damage to your gut caused by glyphosate and other agrochemicals.
Chances are, if your glyphosate levels are high, you probably have a number of other pesticides in your system as well. Fermented foods, particularly kimchi, are potent chelators of these kinds of chemicals. Taking activated charcoal after a questionable meal can help bind and excrete chemicals as well. Remember to stay well-hydrated to facilitate the removal of toxins through your liver, kidneys and skin.
Glycine is an important detox aid for glyphosate in particular. Dr. Dietrich Klinghardt, recognized as an international authority on metal toxicity and its connection with chronic infections, recommends taking 1 teaspoon (4 grams) of glycine powder twice a day for a few weeks and then lower the dose to one-fourth teaspoon (1 gram) twice a day.
The least expensive way to do this is purchase glycine bulk powder,82 which is very inexpensive. This forces the glyphosate out of your system, allowing it to be eliminated through your urine. Using a sauna on a regular basis is also recommended to help eliminate both pesticides and heavy metals you may have accumulated.
Organic Food Resources
While most people tend to think of organics only in terms of produce (fruits and vegetables), it’s important to remember to buy organic, grass fed beef, poultry and dairy, as well, as conventionally raised animals are routinely fed a diet of genetically engineered grains that are loaded with glyphosate and other potentially hazardous ingredients. If you live in the U.S., the following organizations can help you locate farm-fresh foods:
Demeter USA — Demeter-USA.org provides a directory of certified Biodynamic farms and brands.
American Grassfed Association (AGA) — The goal of the American Grassfed Association is to promote the grass fed industry through government relations, research, concept marketing and public education.
Their website also allows you to search for AGA approved producers certified according to strict standards that include being raised on a diet of 100% forage; raised on pasture and never confined to a feedlot; never treated with antibiotics or hormones; and born and raised on American family farms.
EatWild.com — EatWild.com provides lists of farmers known to produce raw dairy products as well as grass fed beef and other farm-fresh produce (although not all are certified organic). Here you can also find information about local farmers markets, as well as local stores and restaurants that sell grass fed products.
Grassfed Exchange — The Grassfed Exchange has a listing of producers selling organic and grass fed meats across the U.S.
Local Harvest — This website will help you find farmers markets, family farms and other sources of sustainably grown food in your area where you can buy produce, grass fed meats and many other goodies.
Eat Well Guide: Wholesome Food from Healthy Animals — The Eat Well Guide is a free online directory of sustainably raised meat, poultry, dairy and eggs from farms, stores, restaurants, inns, hotels and online outlets in the United States and Canada.
The Cornucopia Institute — The Cornucopia Institute maintains web-based tools rating all certified organic brands of eggs, dairy products and other commodities, based on their ethical sourcing and authentic farming practices separating CAFO “organic” production from authentic organic practices.
RealMilk.com — If you’re still unsure of where to find raw milk, check out Raw-Milk-Facts.com and RealMilk.com. They can tell you what the status is for legality in your state, and provide a listing of raw dairy farms in your area. The Farm to Consumer Legal Defense Fund83 also provides a state-by-state review of raw milk laws.84 California residents can also find raw milk retailers using the store locator available at www.OrganicPastures.com.
Google will clearly label healthcare facilities that provide abortions in Search and Maps to reduce confusion among users looking for the procedure.
The change comes months after Congressional Democrats pushed the tech giant to better differentiate between abortion clinics and crisis pregnancy centers, which try to dissuade people from seeking abortions and may not offer accurate medical information.
As part of the update, Google will label facilities that are verified to offer abortions with “provides abortions” in results, while other locations will say “might not provide abortions.”
“When someone in the US searches for health care providers that provide abortions — for example, using the query ‘abortion clinics near me’ — the Local Search results box will display facilities that have been verified to provide abortions,” Mark Isakowitz, Google vice president of government affairs and public policy for the U.S. and Canada, wrote in a response letter to Sen. Mark Warner and Rep. Elissa Slotkin.
“People will be able to broaden their search to show other relevant listings (including from organizations that do not provide abortions).”
WHY IT MATTERS
It’s not uncommon for patients looking for abortion services to find misleading information when searching online. According to a Bloomberg News investigation published earlier this month, people seeking abortion providers are “routinely” directed to crisis pregnancy centers on Google Maps.
Google’s label update comes just days after review site Yelp announced it would flag crisis pregnancy center listings to distinguish them from clinics and healthcare facilities that offer abortions.
In the wake of the Dobbs decision overturning Roe v. Wade, privacy experts have raised concerns about how personal data could be used to determine if a user sought an abortion in states where the procedure is now illegal.
In July, Google said it would automatically delete location history when users visit sensitive places like abortion clinics. Period tracking apps, which analyses have noted often share data with third parties, rushed to put out statements about privacy after the Supreme Court decision. Flo launched an “anonymous mode” it said would allow people to use the app without personal email, name and technical identifiers.