
There’s a Superfood Growing in Your Garden


[ad_1]
Enzymes are proteins composed of individual amino acids. They are necessary to speed up many cellular functions and biological processes. Your body secretes enzymes to catalyze biological reactions, making them vital to good health and longevity.1
Each enzyme has a different function, for example, superoxide dismutase, glutathione peroxidase and catalase have antioxidant functions.2 Digestive enzymes such as protease, lipase and amylase are needed for digestion and nutrient absorption and elimination,3 while molecular motor enzymes such as myosin and actin are needed for the activation of muscle contractions.4
The featured lecture reviews the fundamentals of what enzymes are, the main types of enzymes found in your body and in supplements, how enzymes are affected by environmental factors such as your body’s pH and temperature, and why they’re so important for health.
An enzyme’s shape is an important key to understanding the benefits of enzyme therapy, because the shape of the protein determines its function. You could liken enzymes to specialized keys cut to fit specific locks, with the locks in this case being biochemical reactions.
Considering the tens of thousands of biochemical reactions occurring in your body at any given time, it stands to reason there are tens of thousands of enzymes. An interesting feature of enzymes is that while they catalyze biochemical reactions, they’re not used up in the reaction. They merely assist and accelerate reactions.
By lowering the amount of energy needed for a reaction to occur, they allow for reactions that otherwise would not be possible, or would be too slow to keep up with your body’s demands. This is also why enzyme deficiencies are thought to contribute to more rapid aging.
Enzymes can be broadly divided into the following categories:5
• Digestive enzymes — These are involved in digestion, the breaking down of foods into nutrients and elimination of waste products. Digestive enzymes are extracellular, meaning they’re found outside your cells. There are five primary digestive enzymes, each designed to help break down different types of food:6
◦ Protease — These enzymes break down protein
◦ Amylase — Amylase breaks down carbohydrates, sugars and starches
◦ Lipase — This enzyme breaks down fats (If you have IBS, cystic fibrosis, celiac disease, no gallbladder or gallbladder dysfunction and/or obesity, you may benefit from higher levels of lipase. Also, be aware that fluoridated water may decrease lipase and protease production7)
◦ Lactase — This one breaks down milk sugar (lactose) in dairy products
◦ Sucrase — Sucrase breaks down sucrose sugars
• Metabolic enzymes8 — These are involved in energy production and detoxification. Metabolic enzymes are intracellular, meaning inside your cells, where they help the cell carry out a variety of functions related to its reproduction and replenishment.
• Food-based enzymes9 — These are what you find in raw, uncooked/unprocessed foods such as fruits, vegetables and fermented foods and/or supplements.
Enzymes found in enzyme supplements used for enzyme therapy are known as hydrolases. As the name implies, they use a water molecule to cut certain bonds along the amino acid chain. Supplemental enzymes can be divided into three basic types:
Enzymes for supplemental use can be sourced from animal, plant and microbial sources. Pancreatic enzymes, for example, which include all three types (protease, lipase and carbohydrase), are typically obtained from the pancreas of cows or pigs.
Proteolytic enzymes such as bromelain and papain are obtained from pineapple and papaya respectively. Enzymes can also be sourced from microbial or fungal sources. This group is the largest, as microbes and fungi can produce hundreds of different types of enzymes.
There are two primary ways of using an enzyme supplement: digestive or systemic, and the difference between them relates to timing. Taken with food, a digestive enzyme will help break down the food into smaller components.
When taken on an empty stomach, the enzymes will pass through your digestive system and enter your blood circulation, and when absorbed systemically, they serve as powerful proteases, dissolving things like fibrin and decreasing inflammation.
That said, whether you’re using enzymes digestively or systemically, enzyme therapy will improve assimilation and elimination of components. In other words, the enzymes will break things down to their smallest constituent parts, making both assimilation of necessary components, and elimination of components your body does not need, easier.
As explained in a report10 by nutraceutical researcher Jon Barron, director of the Baseline Health Foundation, proteolytic enzymes taken for systemic benefit, meaning on an empty stomach, can help eliminate pathogens, allergens and rogue cells by destroying and digesting their protein-based shield. Systemically, proteolytic enzymes also have the ability to interfere with enzyme production caused by certain cancers, thereby slowing down the cancer’s growth.
In your gut, proteases or proteolytic enzymes, which break down dietary protein and protein-based foreign bodies, function as digestive aids. In your blood, however, they act as blood cleansers that combat inflammation and rebalance your immune system by:11
1. Breaking down foreign proteins in your blood that cause inflammation
2. Facilitating the removal of inflammatory proteins via your blood stream and lymphatic system
3. Reducing edema in inflamed region
4. Significantly increasing the potency of macrophages and killer cells
5. Removing fibrin that prolongs inflammation. Fibrin is a clotting material that restricts blood flow, found both in your blood stream and connective tissue such as your muscles. Cancer cells also hide under a cloak of fibrin to escape detection.12
Once the cancer cells are “uncloaked,” they can be spotted and attacked by your immune system. It is also thought that fibrin makes cancer cells clump together, which increases the chance for metastases.
Fibrin accumulation is also responsible for scar tissue in damaged muscle or at a surgical site. If the buildup is excessive, which can easily occur if your blood flow is poor due to low enzymatic activity, then the scar tissue may lead to chronic problems.
Excess fibrin in your blood may also raise your risk for a heart attack and/or stroke. Symptoms of excess fibrin include: chronic fatigue, poor healing ability, inflammation, pain and high blood pressure
Enzymes are measured13 in units called food chemical codex (FCC units) of some type of assay, such as hemoglobin unit tyrosine base (HUT). The FCC unit is essentially a measure of the enzyme’s functionality — how well it functions under a specific assay or test.
The example given in the lecture is protease having a measure of 50,000 HUT, which means the protease can break down 50,000 bonds of red blood cells under certain laboratory conditions.
This is important to look for when shopping for an enzyme, as the FCC units are a guarantee of a certain level of activity. Simply knowing the weight or mass of an enzyme doesn’t tell you anything about its functionality, as its activity could theoretically be zero.
As noted in the video presentation, environmental factors such as the pH level and temperature inside your body can affect the activity of enzymes. As your temperature rises, enzyme activity will typically increase. If the temperature gets too high, however, the enzyme will break down.
The reason for this is because the positive and negative charges of the amino acid bonds that give the enzyme its shape cause it to vibrate. As the temperature increases, this vibration speeds up, making the enzyme work harder. This is essentially what happens when you have a fever. As your temperature rises, your enzymes start going into overdrive to heal your body.
At a certain vibrational rate, however, it’s simply vibrating too quickly to remain stable, causing it to break apart. This is not a concern for most supplements though, as most remain viable up to 120 degrees Fahrenheit, and the inside of your body will never get that high. Improper storage, on the other hand, could inactivate the enzymes in the supplement if it gets too hot.
As you’d expect, with lower temperature, enzymatic activity decreases. Many will store their enzyme supplement in the refrigerator or freezer for this reason, but this actually isn’t a good idea. The reason? Because taking the bottle in and out of the fridge or freezer could introduce moisture, and this moisture (water) will activate the enzymes.
The best place to store your enzyme supplement is in a relatively cool, dry area such as a kitchen cabinet or pantry. Properly stored, an enzyme supplement will typically retain full potency for up to a year.
The other factor that affects enzyme activity is your body’s pH (acidity versus alkalinity), which changes throughout your digestive tract. As a result, a particular enzyme will be most active or effective in a particular part of your digestive tract, and less active in others.
For this reason, high-quality supplements will contain enzymes with a wide range of pH tolerance, thereby allowing the supplement to perform optimally all the way through your gastrointestinal tract.
As mentioned, your body naturally produces enzymes. So, why would you ever need an enzyme supplement? While it’s true your body continually produces enzymes, certain factors can limit this capacity:
• Aging — Loss of enzyme activity is part of the aging process.
• Genetics — The blueprints in your DNA instruct your cells on which enzymes to make and how much, so genetic anomalies can affect your body’s ability to produce certain enzymes. One example is lactose intolerance — the limited ability to hydrolyze or break down lactose, the sugar found in milk, due to an insufficiency of lactase, the enzyme that breaks down lactose.
• Lifestyle choices — Examples of choices that affect your enzyme capacity include the types of foods you choose to eat (whole food versus junk food, for example, or a vegan versus carnivore diet), the amount of food you eat (too much or too little) and whether or not you choose to fast or smoke.
While aging is inevitable and genetics cannot be altered, you still have a great degree of influence over your enzymes via your lifestyle choices. The healthier your lifestyle, the better your enzymatic activity will be, even without assistance from a supplement.
For example, eating plenty of fresh, raw and/or fermented foods will supply your body with healthy enzymes. Sprouts are a particularly excellent source of live enzymes.
Fasting has also been shown to conserve enzymes. If you do not eat, you will not produce digestive enzymes, allowing metabolic enzyme production and activity to proliferate instead. A supplement can still be valuable, however, to counteract genetics, aging and a less than ideal lifestyle.
When you swallow a food, it first enters the upper portion of your stomach. Here, any enzymes inherent in the food itself start to activate, helping to break the food down. As you might expect, the more the food can be broken down here in the first stage of your gastrointestinal tract, the less labor intensive the digestive process will be later on.
The pH in this upper stomach portion typically ranges from 4 to 6, i.e., slightly acidic. As food enters your stomach, proton pumps lining the lower pyloric part of your stomach starts pumping in hydrochloric acid, and it does this in proportion to the amount of food that you eat. The more food you put in, the more hydrochloric acid is being pumped in to help break down and liquefy that food.
Importantly, hydrochloric acid does not actually help you digest your food. Rather, it activates an enzyme called pepsin, a proteolytic enzyme that helps digest protein. In this lower section of your stomach, the pH ranges from 2 to 4.
As the food is liquefied, it starts dripping into the duodenum, the upper part of your small intestine, triggering your pancreas to secrete alkaline bicarbonates, thereby neutralizing the acidity. The pH of your small intestine typically ranges from 8 to 9.
Pancreatic enzymes are also released, which continue the process of breaking the food down into even smaller constituent parts. In summary, digestion can occur in three areas — your upper stomach, lower stomach and small intestine — and your food choices can significantly influence where and how well digestion occurs in these areas.
Enzyme supplements can also influence digestion in each of these areas, and help optimize assimilation and elimination of the foods you eat. As mentioned, for optimal benefit, you want a supplement capable of working in a wide range of pH levels, as your stomach and small intestine ranges from 2 on the acidic side to about 9 on the alkaline side.
More often than not, taking a blend of enzymes is also beneficial, as no single enzyme can perform all the necessary functions throughout your digestive tract. As noted in the featured lecture, “the better the blend, the better the breakdown of the substrate” into single, di- and tri-chain amino acids.
In summary, factors you want to look for when buying an enzyme supplement are:
While proteolytic enzymes are well-tolerated and safe for long-term use in most people, there are exceptions. If any of the following scenarios apply to you, you should not take proteolytic enzymes:14
|
You’re on prescription blood thinners such as Coumadin, Heparin or Plavix |
|
You’re having surgery within two weeks (as they can increase surgical bleeding) |
|
You have a stomach ulcer |
|
You’re pregnant or lactating |
|
You’re currently taking antibiotics |
|
You’ve had an allergic reaction to pineapple or papaya |
If you’re currently taking a nonsteroidal anti-inflammatory drug for pain and want to add a systemic enzyme, be sure to take them at least one hour apart from each other.
Systemic enzymes are in many ways preferable to painkillers since they effectively lower inflammation and support your body’s innate ability to heal itself, while pain medication simply masks the symptoms while raising your risk for addiction and death.
[ad_2]
Source link


[ad_1]
For decades, robotic technologies have been changing medical procedures and health care for the better. Now, advanced robotic technology has come to knee replacement surgery. But what does this mean for you if you need a knee replacement? What does this mean for orthopedic surgeons?
Knee replacements are already one of the safest and most successful surgeries, with low risks of complications and quality-of-life improvements that can last for many years. Even still, it’s possible that robotic-assisted knee replacements may further improve patient outcomes and satisfaction.
We spoke to Dr. Christine Pui, an orthopedic surgeon at TRIA, to learn what robotic knee surgery is, when it’s used and the possible benefits compared to traditional knee surgery.
When we talk about “robotic” knee replacements, we’re referring to how the procedure is done – not the type of artificial joint that’s implanted. In other words, you will not have a robotic knee joint after surgery.
Instead, robotic knee replacement is a procedure that uses a robotic technology to improve accuracy and precision during knee replacement. At TRIA, we use the ROSA® Knee System, a robotic surgical assistant.
And, if you’re wondering if the robot performs the surgery on its own, the answer is no.
“The robot assists me in performing the surgery – it doesn’t do the surgery itself,” said Dr. Pui.
In fact, the role of the robotic assistant is to provide surgeons with real-time information to make sure the new joint is precisely placed based on the patient’s unique anatomy. But while the robot provides a guide for greater precision, your doctor still needs to be a skilled surgeon. That’s why it’s so important to work with an orthopedic surgeon who’s experienced in total knee replacements.
Robotic technology isn’t a new technology. In fact, back in 2006, surgeons performing a partial knee replacement were the first to use robotic-arm-assisted technology. Since then, millions of robotic-assisted procedures have been done on different parts of the body.
“They keep making refinements in terms of the technology,” Dr. Pui said. “We’ve been waiting for robotic technology to get to the point where it makes sense for our patients – and now it has.”
“By investing in this technology, we’re able to provide another option that’s not widely available within other health care systems,” she added.
“Fundamentally, a robotic-assisted knee replacement is the same procedure as traditional knee surgery,” Dr. Pui said. “The only difference is the technology we use.”
During all knee replacement surgeries, the damaged bone and cartilage is removed from the joint and kneecap before an artificial joint – which is made of metal alloys, high-grade plastics and polymers – is implanted.
Using robotic technology allows doctors to be more precise and accurate when making surgical bone cuts, releasing soft tissue and positioning the implant. This is because doctors have more information to work with.
Before a knee replacement using ROSA, X-rays of your knee are taken to get detailed information about your specific anatomy. These X-rays are used to plan out the procedure, including the best locations for the surgical cuts and knee implant.
Then, during the procedure, ROSA uses cameras and optical lens tracking to follow the exact position of your leg.
“If your leg moves – even just slightly – the robot adjusts so that the surgery is as precise and accurate as possible,” said Dr. Pui. “We can change the measure of the cuts by as little as one millimeter to achieve exactly what we want.”
If you’re a candidate for a total knee replacement, it’s likely that a robotic-assisted procedure is an option for you.
“Anybody can have a robotic knee surgery,” said. Dr. Pui. “But it’s especially good for patients with challenging needs, trauma or prior surgeries to their knees. Surgery in those situations can be very difficult, and I anticipate that the robot would be very helpful.”
In particular, a robotic-assisted knee replacement may be a great choice if you have:
It’s too early to say if robotic-assisted knee replacement surgery delivers better results than traditional surgical methods. But what we can say is that we expect robotic technology to continue to improve.
“It’s kind of the wave of the future,” Dr. Pui said. “The more data we get from performing robotic-assisted surgeries, the more we’ll be able to refine the procedure. And hopefully, patient satisfaction levels will continue to improve, too.”
We’ve touched on a few of these things already, but here’s what we know so far about the possible advantages of robotic knee surgery:
ROSA helps surgeons perform knee replacements with greater surgical precision, which means the surgery may disrupt less bone and tissue. This also means that it may take you less time to heal.
Every person’s knees are unique. Systems like ROSA allow a surgeon to tailor the knee replacement for each person’s anatomy, which may result in a better fit and more natural feeling.
“One thing ROSA does is collect a lot of data which helps us gauge how the knee is going to function,” said Dr. Pui. “ROSA helps make sure the knee is a good fit with good balance. This can hopefully help the artificial knee feel more natural for the patient.”
For both robotic-assisted knee replacement surgery and traditional surgery, you’ll need time to heal. You’ll also need physical therapy to help you regain strength and mobility. You might also take medication for a couple weeks to help manage pain while you recover.
With robotic-assisted surgery, it’s possible that you may have a shorter recovery time. With the traditional approach, it takes about 4-6 weeks for patients to resume normal activities like driving or going to work. But some of our patients who’ve had a robotic-assisted procedure were back to activities in about half the time.
Knee replacement procedures have a very high success rate. In one study, 96% of implants lasted for more than 10 years with 90% lasting for 20 years. But patient satisfaction rates tell a slightly different story.
“The data out there shows that about 85% of people are really happy with their knee replacements versus total hips, which is more like 95%,” she said. “One of the things we’re trying to achieve through ROSA is to increase patient satisfaction with their knee replacements.”
Frances, who’s 74, lived with knee pain for about 10 years. But when she couldn’t walk for more than a few minutes, she made an appointment with Dr. Pui and they decided the best thing was a knee replacement – with the help of the robotic assistant.
Frances was a little worried about the recovery process. She thought it would take a long time to get back to normal activities and that she would be in pain.
But that wasn’t Frances’ experience. Instead, when she woke up after her knee replacement procedure, she was hardly in any pain. After 3-4 days she stopped taking the pain medication except at night.
She was much more mobile more quickly than anyone would have expected.
“When I would walk into places they were like, ‘Really you just had it done a week ago?’” said Frances.
She’s happy that she had a robotic-assisted knee replacement surgery and knows that her doctor is a huge part of her success.
“Every time I hear horror stories about the pain, I just want to find Dr. Pui and give her a hug,” said Frances.
These days, Frances is living life on her terms.
“Do I have pain? Yeah, every once in a while,” she said. “It will last maybe a few minutes, but it goes away. And I just feel like it’s healing.”
Robotic knee surgery has the same risks of traditional knee surgery, including infection, knee stiffness, ongoing knee pain or an implant that doesn’t work the way the patient and doctor hoped it would.
Complication rates with traditional knee replacement surgery are low – 95% of people don’t have problems. We don’t yet know if robotic surgery will further reduce your chance of complications.
If you’re considering a knee replacement and wondering if a robotic-assisted surgery is right for you, make an appointment with an orthopedic doctor at TRIA.
During the appointment, your doctor will examine your knee, ask you about what you’re experiencing and how you’re currently managing your symptoms. They may also order tests like an X-ray or MRI to see what’s happening inside your knee.
Another big part of this appointment is discussing what your goals are, and if surgery may be the best way to help you meet them. For example, there may be nonsurgical treatment options for knee pain you haven’t tried yet.
If surgery seems like a good option, your doctor will talk to you about scheduling, risks and recovery. They may ask if you’re interested in robotic-assisted surgery. But, if they don’t, feel free to bring it up if you’re interested.
All health plans are required to cover robotic-assisted knee surgery. Still, it’s a good idea to check with your health plan to see how much of the procedure they’ll cover.
Deciding on a knee replacement is a big decision, and thankfully it’s not one you need to make alone. We’ll be there every step of the way, offering guidance and support – from your first consultation through recovery.
[ad_2]
Source link


[ad_1]
Nothing puts a damper on a beautiful summer day like getting stung by a bee, wasp, hornet or yellowjacket (all of which we classify under the term “bee sting”). Fortunately, bee sting treatment is usually straightforward. Home remedies and some over-the-counter first aid items are typically all you need to care for your bee sting.
With the right steps and remedies, you can be back outside enjoying the sunshine in no time at all. Read on to learn what bee stings look like, what treatments can help and when to worry about allergic reactions.
Note: If you are having a severe allergic reaction (anaphylaxis), which can be characterized by swelling in your face and throat, fainting, nausea, difficulty breathing or loss of consciousness, call 911 to seek emergency treatment immediately.
Most people know when they’ve been stung by a bee. It hurts. Plus, the culprit is usually nearby, or it left its stinger behind. But sometimes, all you know is that something stung or bit you. This is especially true for young children.
Toddlers may not have the skills to tell you what happened, but they sure can alert you to the place where it hurts. That’s why it’s important to know what a bee sting looks like. After all, you need to be sure you’re treating the right sting.
Your body can react in one of four ways to getting stung by a bee.
Most of us will experience a local or large local reaction to a bee sting. These are handily treated on your own with first aid and home remedies.
Bee stings hurt. Anyone who says otherwise is probably just trying to impress you. When you get stung by a bee, expect these common symptoms
If your bee sting has caused a local reaction, there’s no need to seek medical care – you can treat it at home. You’ll first need to remove the stinger, if it’s there, and then focus on treating the sting. If you’re unsure of what to do at any step of the way, you can always call our nurse line for helpful tips and reassurance.
Fun fact: One way to know what kind of insect stung you is to check for a stinger. If you’ve got one stuck in your skin, you were stung by a honeybee. A honeybee is the only species with a stinger that detaches, which means that the honeybee will sting and then die. On the other hand, wasps, hornets and other types of bees will fly off to sting again (and again and again).
A stinger will look like a small brown or black dot in the middle of your sting. It will have tiny barbs on it, keeping it lodged in your skin, and perhaps even a venom sac. Don’t worry about looking too closely, just try to get it out as quickly and completely as you can. You can use tweezers, your fingernails (only after you wash your hands), scrape the edge of a credit card across it, or even use sticky tape to remove the stinger. And if you don’t get all of it, it’s not the end of the world – the rest will come out naturally over a little time.
There are a lot of ways to treat bee stings at home, and with items you probably have in your bathroom cabinet or kitchen first aid kit. One of the best things you can do to treat a bee sting at home is use a cold pack or an ice cube to massage the sting. Leave the cold on for 10 minutes at a time and repeat as needed. This will reduce the pain as well as the swelling.
Another home remedy that you could try is honey. Strangely enough, honey seems to soothe angry bee stings. When you consider that honey is often the base ingredient to many homemade drawing salves, there could be more to this treatment method than we give it credit for.
What about mud? Mud is a common home remedy, however mud contains a lot of germs and may even contain tetanus spores. It’s an unsafe home remedy that you should avoid.
If you’re looking for solutions that are more tested than the home remedies mentioned above, you’ve got options, including pain and allergy medications.
You’ve done your best to treat your bee sting at home, followed all the advice and even consulted our nurse line to be sure you were on the right track. So, when can you expect this bee sting to get better? The short answer is 3-7 days. In that time, you will likely experience:
Rarely, through scratching or other outside irritation, a bee sting can become infected. An infected bee sting will have a gooey yellowish-brown crust or scab covering the top of it. The scab may weep or drain yellow fluid.
To treat an infected bee sting, be sure to keep it clean. This will help it get better at home.
With this treatment, you can expect your infected bee sting to improve within 2-3 days and be completely healed within 7-10 days.
Having been stung by a bee once, you’re undoubtedly motivated to not let it happen again. Here are a few quick tips for avoiding stings in the future:

Very rarely, toxic and allergic reactions can occur when you’re stung by a bee. They’re both potentially life threatening, but can be effectively treated when caught early and in the right circumstances.
A toxic reaction to a bee sting happens when a person has the very bad luck of getting stung multiple times. Someone who’s experiencing a toxic reaction may feel nauseous, vomit and develop diarrhea. Within 24 hours, muscle breakdown and renal failure may occur if left untreated. It’s estimated that around 500 stings are enough bee venom to cause death.
Only 0.04% of the population will experience an anaphylactic reaction to a bee sting. It can happen with just one sting, and usually starts within 20 minutes. If you haven’t experienced symptoms within two hours, the chances of you developing anaphylaxis are slim. Symptoms include:
Always call 911 in the event of suspected anaphylaxis. It’s important to note that if you have experienced anaphylaxis in the past, you have a 25-65% chance of experiencing it again if you’re stung.
Call 911 immediately if someone stung by a bee has any of the symptoms mentioned above or has had a life-threatening reaction to a sting in the past.
Visit the emergency department or urgent care if you experience any of the following within two hours of being stung:
Visit urgent care or primary care if you’re experiencing:
Call your doctor or the nurse helpline if:
The best bee sting treatments and remedies are probably right in your own home. From ointments to cold packs, everything you need to treat these pesky stings is likely in your cupboard. But we’re here if you have any questions or need advice. You can call our nurse line or make an appointment with one of our primary care doctors.
Now that you know what to look for, keep an eye out for warning signs of an allergic reaction to bee stings. Knowing what to look for and how to treat bee stings could just save a life.
[ad_2]
Source link


[ad_1]
Like many other conditions, gum disease can be sneaky. In its earliest stages, you may not notice anything has changed with your teeth or gums – especially if it’s been a while since your last dental checkup.
So, what exactly is gum disease and what symptoms might you be able to spot? Keep reading to get the answers to these questions and more.
Gum disease, also called periodontal disease, is an infection of the gums and other tissues surrounding the teeth.
Gum disease can occur when too much plaque builds up on teeth. Our mouths are always forming plaque, which contains bacteria that feed on the sugar and starches in the things we eat and drink. Without good oral hygiene habits, diet and regular dental checkups, plaque builds up and hardens, which is called tartar or calculus.
Once tartar has formed, it acts as a “home” for bacteria. This allows bacteria to grow and continuously expose your teeth and any surrounding tissue to acid, which can lead to inflammation. This can also cause mechanical irritation to your gums, which can lead to ulcers. Inflammation can eventually start to break down the affected tissues and bone, giving bacteria more room to grow, and damaging your teeth and gums.
There are two different stages of gum disease: gingivitis and periodontitis.
Gingivitis is the earliest stage of gum disease, where symptoms are usually mild and limited to the tissues surrounding the teeth. If gum disease is caught and treated at this stage, it usually can be treated without major damage to your gums. But if left untreated, it can progress into periodontitis.
Periodontitis is more severe gum disease where infection has spread below the gums, damaging the tissues and bone that support the teeth. There are three stages of periodontitis disease: early periodontitis, moderate periodontitis and advanced periodontitis. There are specific markers for each stage, which are used by dentists during diagnosis.
The early stages of gum disease often don’t involve any pain or discomfort. This makes it important to look out for other signs like visual changes to your gums or teeth. The longer gum disease is left untreated, the more damage it can cause and the more costly it can be to treat. So if you notice one or more of the symptoms below, it’s best to see a dentist as soon as possible.
Healthy gums are light pink, firm and fit tightly around teeth, while infected gums can be:
The most common signs of early gum disease are:
In addition to the early signs above, symptoms of more advanced gum disease include:
To diagnose gum disease, a dentist will examine your mouth for symptoms like tartar buildup, easy bleeding and receding gums. They’ll also review your dental and medical histories for possible risk factors.
A dentist may also use a dental probe as part of the diagnosis, and to determine what stage of gum disease you have. This is done by measuring the depth of the spaces (or pockets) between your teeth and your gums, and checking for any loss of the connective tissue that holds your teeth in their sockets. X-rays may also be taken to check for bone loss around them.
Good oral hygiene is key to preventing gum disease. For your daily life, this means brushing at least twice a day and flossing between your teeth once a day. But good oral hygiene also means following a dentist-recommended schedule of regular dental checkups. These checkups are opportunities to get your teeth cleaned more deeply than you can clean them at home, and they also allow your dentist to catch and treat signs of oral health issues like gum disease before they become severe.
In addition, there are lifestyle factors that can help keep your mouth healthy. Two of the biggest are:
Gum disease that’s progressed beyond gingivitis requires professional treatment, but successful treatment depends on you, too.
To make sure gum disease doesn’t come back in the future, it’s important to address any risk factors you have, in the same way that you would if you were trying to prevent it in the first place. This could include improving your oral hygiene, changing your diet, losing weight, quitting smoking or managing chronic health conditions like diabetes.
Professional treatment for less advanced cases of gum disease typically involves root planing and scaling (deep cleaning). Planing and scaling may take multiple visits to complete. At HealthPartners Dental, we provide a local anesthesia or anesthetic rinses to help keep our patients comfortable during deep cleanings.
If you’re noticing pain in your mouth, bleeding gums or other unusual symptoms, don’t ignore them. Without treatment, gum disease may advance and lead to more painful and costly dental problems. A dentist can examine your mouth for issues, provide the exact treatment you need and offer expert recommendations that will help keep your teeth strong and healthy for years to come.
[ad_2]
Source link


[ad_1]
Red, swollen or tender gums. Bad breath that doesn’t go away. Bleeding when you brush or floss. While any of these mild symptoms could be ignored, if you’re noticing them regularly it’s time to pay attention.
That’s because they could be early symptoms of gum disease , which is called gingivitis. If left untreated, gingivitis can lead to more serious gum disease and dental issues. But the good news is that gingivitis is completely reversible if it’s caught and treated early.
Gingivitis is most commonly caused by insufficient oral hygiene such as not brushing enough, not flossing enough or not having regular dental checkups. Without good oral hygiene, plaque builds up on your teeth, and can harden into tartar. Plaque and tartar contain bacteria, and these bacteria can damage your gingiva, leading to inflammation.
Symptoms of gingivitis can include one or more of the following:
Having one or more of the above symptoms is reason to see a dentist. But in general, any amount of pain or bleeding in your mouth means it’s time to make an appointment. It can be easy to ignore a little irritation, but it’s important to treat oral health conditions like gingivitis as early as possible.
To diagnose gingivitis, a dentist will closely examine your teeth and gums for signs of inflammation, recession and more. They may also ask you questions about your medical and dental histories to find out if you have any risk factors for gingivitis, such as tobacco use or a family history of gum disease.
The dentist or dental hygienist may also measure the depth of the spaces or “pockets” between your teeth and the gum tissue surrounding them. Pockets in a healthy mouth are generally 1-3 millimeters deep. X-rays may also be taken to check for any bone loss.
Generally, yes. If gingivitis is caught early, before any permanent damage has occurred, your gums can recover.
Taking steps to improve your oral hygiene can certainly help reduce gingivitis symptoms. But a dental exam is needed to determine how advanced gum disease is. For example, plaque can be removed with good brushing and flossing, but tarter buildup needs to be removed by a dental hygienist.
There are several oral hygiene habits and lifestyle changes you can make to prevent gingivitis from developing or coming back, including:
In addition to the steps you take on your own, a dentist may treat gingivitis with:
If left untreated, gingivitis can develop into more advanced gum disease, which is known as periodontitis. Symptoms of periodontitis are more severe, and it can lead to serious infection, bone loss and tooth loss.
Oral health issues are best treated early, before they become more painful and expensive. So if you’re noticing changes in your mouth that could be signs of gingivitis, or if you have any other concerns about your oral health, making an appointment with a dentist is your next step.
At your appointment, you’ll receive a dental exam, and your dentist will work with you to address any oral health concerns you have.
[ad_2]
Source link


[ad_1]
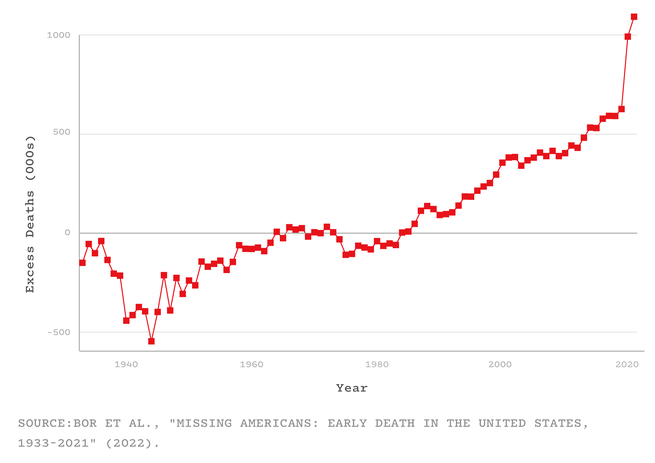
Jacob Bor has been thinking about a parallel universe. He envisions a world in which America has health on par with that of other wealthy nations, and is not an embarrassing outlier that, despite spending more on health care than any other country, has shorter life spans, higher rates of chronic disease and maternal mortality, and fewer doctors per capita than its peers. Bor, an epidemiologist at Boston University School of Public Health, imagines the people who are still alive in that other world but who died in ours. He calls such people “missing Americans.” And he calculates that in 2021 alone, there were 1.1 million of them.
Bor and his colleagues arrived at that number by using data from an international mortality database and the CDC. For every year from 1933 to 2021, they compared America’s mortality rates with the average of Canada, Japan, and 16 Western European nations (adjusting for age and population). They showed that from the 1980s onward, the U.S. started falling behind its peers. By 2019, the number of missing Americans had grown to 626,000. After COVID arrived, that statistic ballooned even further—to 992,000 in 2020, and to 1.1 million in 2021. Were the U.S. “just average compared to other wealthy countries, not even the best performer, fully a third of all deaths last year would have been prevented,” Bor told me. That includes half of all deaths among working-age adults. “Think of two people you might know under 65 who died last year: One of them might still be alive,” he said. “It raises the hairs on the back of my neck.”
These counterfactuals puncture two common myths about America’s pandemic experience: that the U.S. was just one unremarkable victim of a crisis that spared no nation and that COVID disrupted a status quo that was strong and worth restoring wholesale. In fact, as one expert predicted in March 2020, the U.S. had the worst outbreak in the industrialized world—not just because of what the Trump and Biden administrations did, but also because of the country’s rotten rootstock. COVID simply did more of what life in America has excelled at for decades: killing Americans in unusually large numbers, and at unusually young ages. “I don’t think people in the United States actually have any awareness of just how poorly we do as a country at letting people live to old age,” Elizabeth Wrigley-Field, a sociologist at the University of Minnesota, told me.
Although Bor’s study has yet to be formally reviewed, Wrigley-Field and five other independent researchers vouched for its quality to me. “The paper is extremely important, and the researchers who produced this know what they’re doing,” Steven Woolf, a population-health expert at Virginia Commonwealth University, told me. “It builds on, and considerably expands, what we’ve already known.”
Several studies, for example, have shown that America’s life expectancy has tailed behind other comparable countries since the 1970s. By 2010, that gap was already 1.9 years. By the end of 2021, it had grown to 5.3. And although many countries took a longevity hit because of COVID, America was once again exceptional: Among its peers, it experienced the largest life-expectancy decline in 2020 and, unlike its peers, continued declining in 2021. But Bor says that people often misinterpret life-expectancy declines, as if they simply represent a few years shaved off the end of a life. Someone might reasonably ask: What’s the big deal if I die at 76 versus 78? But in fact, life expectancy is falling behind other wealthy nations in large part because a lot of Americans are dying very young—in their 40s and 50s, rather than their 70s and 80s. The country is experiencing what Bor and his colleagues call “a crisis of early death”—a long-simmering tragedy that COVID took to a furious boil.
In every country, the coronavirus wrought greater damage upon the bodies of the elderly than the young. But this well-known trend hides a less obvious one: During the pandemic, half of the U.S.’s excess deaths—the missing Americans—were under 65 years old. Even though working-age Americans were less likely to die of COVID than older Americans, they fared considerably worse than similarly aged people in other countries. From 2019 to 2021, the number of working-age Americans who died increased by 233,000—and nine in 10 of those deaths wouldn’t have happened if the U.S. had mortality rates on par with its peers. “This is a damning finding,” Oni Blackstock, the founder and executive director of Health Justice, told me.
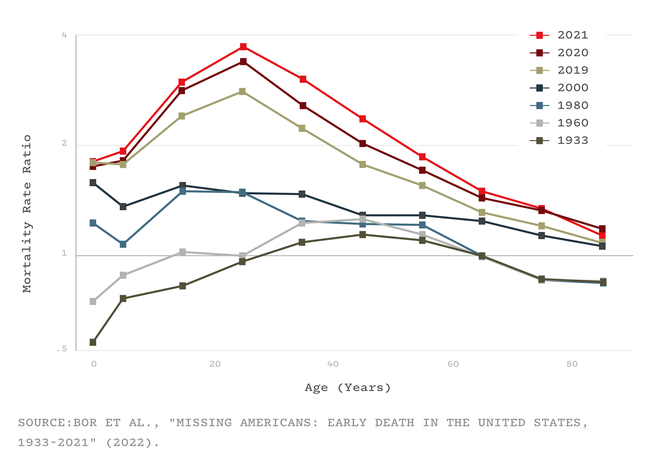
The crisis of early death was evident well before COVID. As many studies and reports have shown, since the turn of the 21st century, “midlife ages are where health and survival in the U.S. really go off the rails,” Wrigley-Field told me. “The U.S. actually does well at keeping people alive once they’re really old,” she said, but it struggles to get its citizens to that point. They might die because of gun violence, car accidents, or heart disease and other metabolic disorders, or drug overdoses, suicides, and other deaths of despair. In all of these, the U.S. does worse than most equivalent countries, both by failing to address these problems directly and by leaving people more vulnerable to them to begin with.
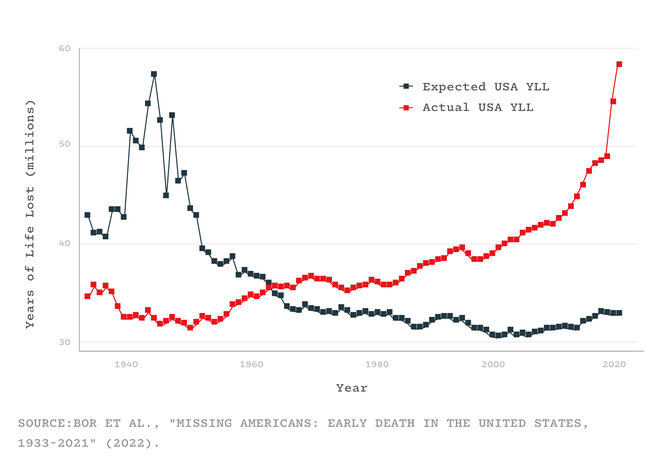
Consider how many years the missing Americans would have collectively enjoyed had they survived—all the birthdays and anniversaries that never happened. In other rich countries, the total “years of life lost” have flatlined for the past five decades. In the U.S., they have soared: In 2021 alone, the 1.1 million missing Americans lost 25 million years of life among them. That number doesn’t account for the events that preceded many of these deaths—the “years of disability, illness, and loss of human potential, creativity, and dignity,” Laudan Aron, a health-policy researcher at the Urban Institute, told me. And, especially in the case of middle-aged deaths, they left behind young dependents, whose own health might suffer as a result. The sheer number of missing Americans, and the “profound ripple effects” of their absence, are “really hard to wrap one’s head around,” Aron said.
These staggering numbers also help contextualize COVID’s toll. The coronavirus caused the largest single-year rise in mortality since World War II, becoming the third leading cause of death in the U.S., after only heart disease and cancer. But this enormous tragedy unfolded against an already tragic backdrop: The number of missing Americans from 2019 is larger than the number of people who were killed by COVID in 2020 or 2021. This isn’t to minimize COVID’s impact; it simply shows that in the Before Times, America had “very successfully normalized to an extremely high level of death on the scale of what we experienced in the pandemic,” Justin Feldman, a social epidemiologist at Harvard, told me. And when COVID drove those levels skyward, America proved that “we’ll accept even more deaths compared to our already poor historical norms,” Feldman said.
Such deaths, though obvious on a graph, are hidden from Americans with social privilege. In the summer of 2020, Bor remembers having an outdoor barbecue with a friend who grew up in a low-income housing project. “At that point, six months in, he knew six people in his close circle who had been killed by COVID,” Bor told me. “I still don’t.” The fact that half of the working-age Americans who died last year should still be alive “isn’t visceral if you haven’t lost anyone,” he said.
The current mortality crisis was long in the making. In terms of mortality, America’s peer countries—many of which had been hammered by World War II and its aftermath—began catching up with it in the mid-1970s before overtaking in the early 1980s. That was a pivotal era, when globalization, automation, and a growing service industry led to huge losses in mining, manufacturing, and other blue-collar sectors. The U.S. profoundly failed to protect its citizens from these changes. Its social safety net—state assistance for parents, or people facing job, food, or housing insecurity—was meager; its public-health system was languishing after decades of underinvestment; and unlike every other wealthy country, it lacked universal health care. These factors “privatized risk,” Bor and his colleagues wrote in their paper, “tying health more closely to personal wealth and employment.” As labor unions declined and minimum wages stagnated, more Americans had fewer resources to lean on if their health declined. Poorer Americans already lived, on average, shorter lives than rich ones, and that gulf started to widen.
Other particularly American choices exacerbated the stresses on the health of the country’s citizens, again weighing more heavily on less wealthy people. A growing mass-incarceration industry punished them. A deregulatory agenda that began with Ronald Reagan’s administration left them vulnerable to unhealthy foods, workplace hazards, environmental pollutants, guns, and opioids. “America basically says: If you’re poor, you don’t have access to safe choices,” Bor told me.
Factors like social inequalities and frayed social safety nets are the fundamental weaknesses of American society, which more specific problems like opioids, metabolic disorders, and COVID exploit. During the pandemic, for example, poor and minority groups were more likely to be infected because they lived in crowded housing, distrusted medical leaders, and couldn’t work from home or take time off when sick. And instead of addressing these foundational problems, policy makers instead focused on personal responsibility.
America’s drastic underperformance in health also stems from its history of segregation and discrimination. Racist policies have obviously harmed the health of minorities. But as the policy expert Heather McGhee and the physician Jonathan Metzl have independently argued, elites have long marshaled the racial resentment of poor white Americans to undermine support for public goods that would benefit everyone, such as universal health care. Per Frederick Douglass and other Black leaders, “They divided both to conquer each.”
COVID, for example, disproportionately killed Black, Latino, and Indigenous Americans—a trend that, when highlighted to white people, reduces their concern about the pandemic and their support for safety measures. But in 2021, young white Americans still died at three times the rate of the average resident of other peer nations, while young Black and Indigenous Americans died at rates five- and eightfold higher, respectively. “There are thousands of racial-disparity studies that compare Black people to white people—but white Americans are a terrible counterfactual,” Bor told me. They’re frogs in the same pot, boiling more slowly but boiling nonetheless. By using them as a baseline, we ignore how “everyone is harmed by the status quo in the U.S.,” Blackstock told me, while also underestimating how dire things really are for people of color. (The same problem applies to income inequality: White Americans living in the richest 1 percent of counties still have higher rates of maternal and infant mortality than the average residents of wealthy countries.)
So, “what happens now?” Bor asked me. “Are we going to have 1 million missing Americans a year, every year, going forward? Or more?” His study doesn’t suggest a reason for optimism, but it does provide a defense against nihilism. The entire concept of missing Americans is rooted in a comparison with other countries, which shows that these early deaths aren’t inevitable. The U.S. could at least start moving in the direction of its peers by adopting policies that work elsewhere, such as universal health care, minimum-wage increases, federally required paid sick leave, and better unemployment insurance.
But “the inability of our politics to generate policies that manage health threats is grim,” Bor said. None of the weaknesses that COVID exposed have been addressed; some, like the chasm-sized health gaps between rich and poor or white and Black, have been widened. Vaccines significantly reduce the risk of dying from COVID, but their power is blunted by low uptake, new variants, the lifting of almost all infection-thwarting protections, and the looming loss of COVID funding. Reactionary laws that hamstring what public-health departments can do in emergencies will make the U.S. vulnerable to the new viruses that will inevitably assault it in future years. America’s already underperforming health-care system has been badly battered by the pandemic, and weakened by waves of health-care-worker resignations. In recent months, the Supreme Court has constrained both gun and carbon-emission regulations, while clearing the road for states to restrict or ban abortions—a move that could easily boost America’s already sky-high maternal mortality rates. The climate is still changing rapidly, exposing people who have no choice but to work outside to the ravages of heat.
As much of the country returns to normal, Bor’s study makes plain what normal actually meant—and, as I wrote in 2020, that normal led to this. “A lot of Americans may be under the impression that we had a bad go of it during COVID, and once the pandemic is over, they can go back to having the best health in the world,” Woolf told me. “That is a gross misconception.”
[ad_2]
Source link


[ad_1]
In early July, Sebastian Kohn, a 39-year-old nonprofit professional in Brooklyn, woke up with a fever, a sore back, and swelling in the lymph nodes of his throat and groin. He took a COVID test, which was negative. But Kohn had some clue as to what might be going on. Pride celebrations had taken place a week earlier, and a newly infamous disease was circulating largely in the gay community: monkeypox.
Suspicious that he might have the viral illness, Kohn immediately isolated. Two days later, a painful, itchy rash appeared in an intimate location. He knew then that he was in for a ride. Kohn found an urgent-care center where a doctor was able to swab his skin lesions and send them off to a lab, where technicians searched for signs of the virus’s genetic material. Then he waited, alone, in his home.
More than 15,000 monkeypox cases have been confirmed around the world since the outbreak began in May, but the condition, which spreads through close contact with the rash or body fluids of an infected individual, has been difficult to diagnose because of a lack of available testing. New York City was at one point able to test only 10 patients a day. When Kohn got sick, the system was still running at significant delays. While an analogous COVID test can be turned around by the next day in many cases, Kohn’s positive result for monkeypox took four days to arrive—all while a blistering rash spread out across his body. (Six days after that, Kohn received a phone call from a contact tracer working for the local department of health. He may have been exposed to monkeypox, the person warned.)
In terms of sheer numbers, the nation’s monkeypox-testing capacity has increased dramatically since Kohn’s run-in with the system. On Monday, the Centers for Disease Control and Prevention announced that the U.S. is now capable of evaluating 80,000 cases a week, up from 6,000 initially. But another, more important bottleneck remains stubbornly in place: The CDC’s official guidance recommends that labs test for monkeypox using only samples of a patient’s skin, taken at the site of a visible rash. As a result, people like Kohn, whose fever and swollen lymph nodes come on a few days before their lesions, must let the illness grow before it can be diagnosed. Others may develop hidden sores in their mouth or anus, and not realize that they can be tested. And many more without symptoms will be left to wait and wonder, after an exposure, whether they might have been infected.
As the outbreak spreads—with more than 2,000 cases in the U.S., by the latest count—public-health authorities have doubled down on this restriction: Testing for the virus must make use of swabs taken from a lesion, according to a “Safety Communication” issued by the Food and Drug Administration last Friday. “The FDA is not aware of clinical data supporting the use of other sample types, such as blood or saliva, for monkeypox virus testing,” the communication said, and testing of these other types “may lead to false test results.” This alarming messaging, delivered at a crucial moment in the virus’s spread, will have a profound effect on how quickly new monkeypox infections can be identified, isolated, and treated.
With this disease, like many others, early detection is invaluable as a means of promoting early treatment. Vaccination shortly after exposure can prevent monkeypox from occurring in many cases, and inoculation during the early phase of illness may reduce the severity of symptoms or curtail the contagious period. Although no medications have been approved specifically for monkeypox, several antivirals originally meant for smallpox are thought to help. As we have seen with the COVID antivirals Paxlovid and remdesivir, these types of therapies tend to work best when given as early as possible.
It may be just as important to identify those infected asymptomatically. An intriguing study out of Belgium, posted earlier this month but not yet peer-reviewed, examined swabs taken from the mouth and anus of 224 men in May. Samples had originally been collected to look for gonorrhea and chlamydia, but the scientists found monkeypox DNA in three of them. None of those men reported any symptoms of disease before or after testing, nor did any of their close contacts. Nevertheless, the study’s authors believe that these and other potential asymptomatic carriers could well be contagious. (Guidance from the CDC, last updated at the end of June, says that spreading can happen only after symptoms start.) In the meantime, other studies, conducted in Europe and Africa, have shown that monkeypox DNA is in many cases detectable in saliva, blood, urine, and rectal samples, even before a rash appears.
Matt Ford, a 30-year-old actor and video producer who lives in Los Angeles and New York, told me that he suspects he passed the virus on during the very early phase of his infection. He caught monkeypox last month, and was subsequently placed under public-health isolation. But in the week between his exposure and when he first noticed skin spots, he said, he spent an evening with a guy he was seeing. That guy would later come down with the disease himself. In retrospect, Ford had been a little tired during that time, but he had not felt unwell enough to pay it any mind. If people really are passing on the virus with few to no symptoms—and we don’t know for sure—then an early-detection test collected by mouth, vein, or rectal swab might prevent this onward spread.
Yet last week’s warning from the FDA was very specific: Unless you have an active rash, don’t bother to get tested. When I asked the agency what specific data it was relying on for its safety communication, an FDA spokesperson repeated only that the organization is “not aware of clinical data supporting asymptomatic testing or testing samples other than those taken directly from a suspect lesion.” CDC Director Rochelle Walensky also confirmed to reporters last week that a skin lesion is required for testing from her organization’s perspective, though she said that the CDC is exploring the possibility of saliva, throat, and blood tests.
This “absence of evidence” maneuver by authorities should be quite familiar at this point. In December 2019 and January 2020, the Chinese government publicly stated that there was no clear evidence of human-to-human transmission of the new coronavirus, and the World Health Organization repeated the claim. Three months later, in April, officials from the WHO cited “no evidence” that wearing masks prevented COVID transmission in a wider community setting. In the case of monkeypox testing, such conservatism is particularly self-defeating. When public-health authorities warn of a lack of clinical data for the effectiveness of blood and saliva tests, they are not only ignoring a small but growing list of published studies; they are also making it that much harder for researchers to collect more clinical data. The FDA and the CDC should be encouraging labs to run and evaluate new tests, Jay Varma, a public-health physician and professor at Cornell, told me. Instead the agencies are telling labs to stay away from them.
The FDA is correct that any new test for monkeypox would almost certainly produce some false results. (Even the gold-standard skin tests for monkeypox can misclassify cases.) But the advantages of having an early diagnostic for monkeypox are beyond dispute: Most people would take precautions to reduce their chance of exposing others if they knew they were infected, and contact tracers could hunt down additional cases far more quickly.
Ideally, one could imagine integrating monkeypox testing into the sexual-health infrastructure that is already in place. Many members of the gay community are used to receiving regular screening for HIV and other sexually transmitted diseases, according to Joseph Osmundson, a clinical assistant professor of biology at NYU. “There is a real desire in the community for scale testing” for monkeypox, too, he told me. Throat and rectal swabs collected for gonorrhea and chlamydia, for example, could also be tested for the virus. Varma suggests checking participants at any event where casual sex is expected to occur.
As things stand, physicians, patients, and laboratories would have to defy the explicit advice of U.S. public-health authorities in order to make this happen. Labs are legally permitted to create their own monkeypox diagnostics, even in the face of the FDA’s official warnings. Indeed, some organizations have already begun doing so. (If the U.S. government were to formally declare monkeypox a public-health emergency—as some politicians are calling for—then, ironically, this regulatory flexibility could be revoked.) Benjamin Pinsky, the medical director of the clinical-virology lab at Stanford, has overseen the testing of more than 70 patients for monkeypox, using samples from the nose, mouth, rectum, and bladder, as well as traditional skin scrapings. The newer methods have already picked up a few cases, he told me, but developing those tests without the cooperation of the government has been difficult. Pinsky said that public-health labs initially refused to provide him with real patient samples to confirm the validity of his approach. Many less-experienced lab directors will be dissuaded entirely from setting up their own protocols, because designing a diagnostic from scratch is far more complicated than using an off-the-shelf tool provided by the government. Also, no lab director would be eager to explain to hospital administrators why he or she is openly flouting an official safety warning.
One need only look back at the COVID testing snafus of 2020 to get a sense of what can happen when the government works against, rather than with, the medical community. At the start of the pandemic, the FDA prohibited labs from developing their own COVID-detection methods without first completing an arduous authorization process. Hospitals were encouraged to rely on the CDC’s official test, just as they are now for monkeypox. The government COVID test turned out to have a serious manufacturing defect, which thankfully hasn’t been repeated during the monkeypox outbreak. But excess caution remains a problem, and has once again left the country dangerously short of diagnostic capacity. U.S. hesitation also puts the country out of step with the international community. The WHO, parts of Canada, and the United Kingdom, for instance, all recommend analyzing a throat swab in some circumstances.
It’s not that the FDA’s concerns are unfounded. A monkeypox-testing bonanza, in which anyone and everyone can start to market their own services with limited oversight, could have undesirable consequences. Once the rules were loosened for COVID tests, small and inexperienced laboratory outfits served up diagnostic errors on occasion, or engaged in exploitative practices. But most labs follow proper quality-control procedures, and the Centers for Medicare and Medicaid Services still provides routine supervision. Any risk of false results in such an environment must be weighed against the more serious consequence of missing cases entirely. Less testing for monkeypox this summer will inevitably lead to more people suffering from ulcerating rashes, drenching night sweats, malodorous rectal discharge, and expansive onward spread.
Members of the gay community want easier and earlier testing for monkeypox. Public-health experts want the same thing. Aggressive case-finding may be the only way to get the current outbreak under control, and most large labs have the ability to detect the presence of monkeypox DNA in a variety of body fluids. We don’t yet know the real-world performance of a monkeypox-screening program based on all these fluids, but doctors could and should be coordinating with one another and with public-health agencies to find out. “We want the best diagnostics, the best vaccines, the best treatment protocols, and the best science in the world,” Osmundson told me. “But we are also in an emergency, and people are getting sick, and they are not able to access the care they need.”
[ad_2]
Source link


[ad_1]
And there it is: President Joe Biden has tested positive for the coronavirus, the White House announced Thursday morning, and is dosing up with Paxlovid to keep his so-far “very mild symptoms” from turning severe.
In some ways, this is one of the cases the entire world has been waiting for—not sadistically, necessarily, but simply because, like so many other infections as of late, it has felt inevitable. Once, it might have seemed possible to avoid this virus; now most Americans have had it. SARS-CoV-2 has been spewing out variants and subvariants at an absolutely blistering clip, and wave after wave of infections has slammed the nation, collapsing case peaks into a never-ending plateau. Vice President Kamala Harris caught the coronavirus in April; Anthony Fauci got it in June.
Perhaps the most notable aspect of these high-profile cases is not that they happened, but when. Though certainly on the front lines of the country’s COVID response, these officials have enjoyed the privilege of protection throughout the pandemic, with access to masks, tests, vaccines, and, most recently, antivirals; the comfort and security of jobs that can be done while in isolation; the socioeconomic means to separate themselves from colleagues and loved ones, and the support staff to alert close contacts about exposures. They, as much as anyone feasibly could, “have had access to all the available tools” the country has to fight the coronavirus, says Anne Sosin, a public-health researcher at Dartmouth College, so much so that they’ve even had the liberty to get a bit avant-garde. Fauci, for instance, received two courses of Paxlovid when his symptoms vanished and then reappeared—an unsanctioned use of the drug that sparked some criticism from infectious-disease experts who thought the move unwarranted and potentially baffling for a public unsure of who should be taking the drug and how.
Avoiding the virus, or at least a known, test-confirmed infection, up until this point of the pandemic does have real value. In the U.S., our collective capability to evade any serious outcome is much higher than it was in, say, October 2020, when then-President Donald Trump tested positive. Trump’s tussle with the virus unfurled at a time before COVID vaccines were available, and his doctors treated his illness as a pressing medical emergency, rushing him to the hospital for observation and treatment. At the time, COVID therapies were focused on the severely sick, and had to be administered by a trained health-care professional, typically in a medical setting; like Biden, Trump got the best care that was available at the time, but in the first year of the crisis, that entailed the trifecta of remdesivir, steroids, and still-experimental monoclonal antibodies, which Trump later touted, misleadingly, as a “cure.” Most monoclonal-antibody treatments, including the specific cocktail Trump received, have since fallen out of use because they’re less effective against the variants circulating today.
Today, President Biden may not need anything beyond Paxlovid, which the FDA greenlit late last year and can be taken as a pill at home. “We know so much more now,” says Taison Bell, a critical-care and infectious-disease physician at UVA Health. “We understand what treatments work, what treatments don’t.” Although Biden is 79—an age that puts him at high risk of severe outcomes from the virus—he’s quadruply vaccinated, having received his second booster in late March. And clinical trials have shown Paxlovid to be nearly 90 percent effective at slashing the risk of COVID hospitalizations or deaths (though those data were gleaned from an entirely unvaccinated population; real-world estimates of the drug’s performance have been far more mixed). Kevin O’Connor, the president’s physician, wrote in a letter today that “I anticipate that he will respond favorably, as most maximally protected patients do.”
In the third year of the pandemic, just as unsurprising as Biden’s illness is the pressure for the White House to leverage it as a statement on the right approach to COVID control. In 2020, Trump alarmed experts by peeling off his mask and walking into the White House just after being discharged from the hospital that treated him for COVID. Nearly two years later, Biden, to begin with, is apparently modeling some version of business as usual: The White House has already announced that he “continues to carry out the full duties of the office while in isolation” … which somehow involves the country’s chief decision maker tweeting out maskless photos (taken by someone else, presumably) of himself doing paperwork at his desk.
But, like Trump’s, Biden’s experience—including any performative professional displays—is still an exception among exceptions. “The president, as we would want, has access to therapies,” says Utibe Essien, a physician and health-equity researcher at the University of Pittsburgh. “We would hope that everyone should.”
They do not. Although the White House has made plenty of noise about the need for funding to keep the country awash in tests, treatments, and vaccines, Congress has not provided those resources, and the administration has not marshaled the political will to change that situation. Nor has it sparked the enthusiasm necessary to reignite America’s pandemic response where it has flagged. Cases remain undercounted; tests remain underused. Vaccination rates—especially boosting rates—remain worrisomely low. Effective treatments have been collecting dust on shelves amid enormous disparities in access. And gathering restrictions and masks are now mostly mitigation measures of the past, even though the CDC’s loosened guidelines currently recommend that people in more than a third of the country’s counties should be covering their face to control the coronavirus’s spread. At the beginning of this month, in a Fourth of July celebration, the president crowed that the country was “closer than ever to declaring our independence from a deadly virus”; weeks later, he is playing host to that same foe. And although he might have had access to the tools needed to combat it, “that doesn’t mean they’re going into the hands of the people who need them,” Essien told me.
That the president’s infection happened now, during the nation’s roiling, months-long, multi-subvariant wave, speaks to the bad cycle that the country has found itself in. The current surge shows few signs of slowing; more iterations of the virus are undoubtedly on their way. And yet little is being done in response to the danger, let alone as a preventive to keep the situation from going further off the rails. The U.S. has defaulted to acceptance, Sosin told me, of the status quo: uncontrolled transmission, viral evolution on loop.
Biden could have delayed his encounter with the disease a bit longer, buying time for the development of even better antivirals, clarity on the risks of long COVID, or, at the very least, fall’s highly anticipated BA.4/5 vaccine update. Doing that, though, would have required more investment—from him, perhaps, as an individual, but in particular from his country, under his leadership, to collectively tamp down transmission. In this current environment, however, “the virus has that many more pathways to spread through the community,” Bell told me—up to and including the president.
[ad_2]
Source link